 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
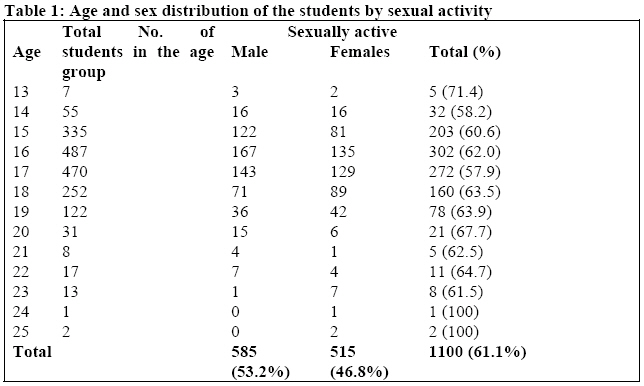
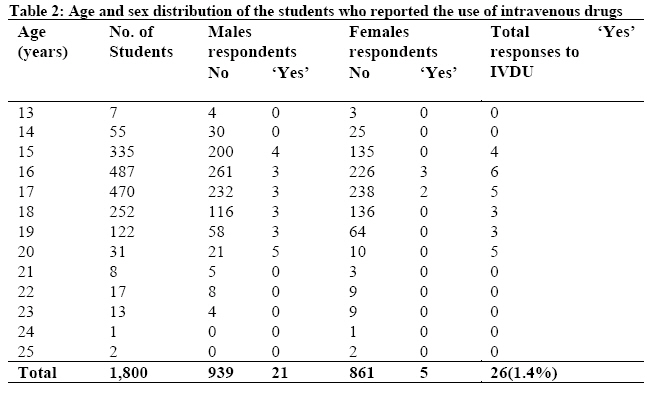
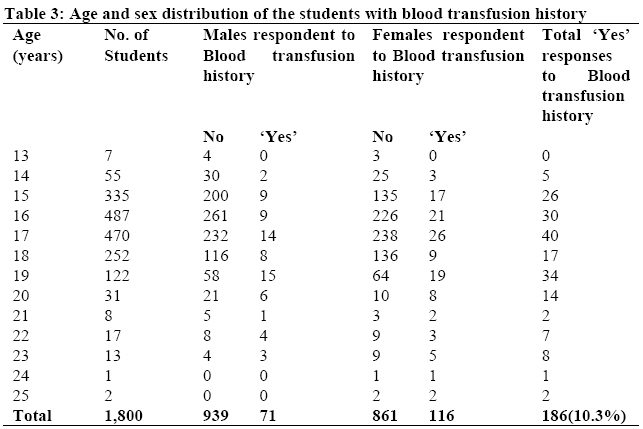
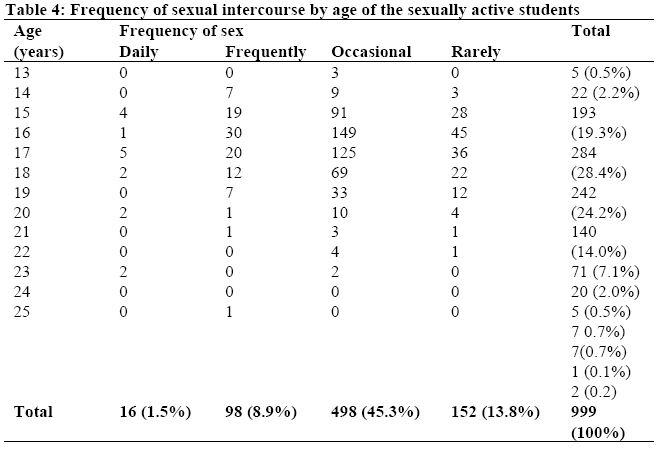
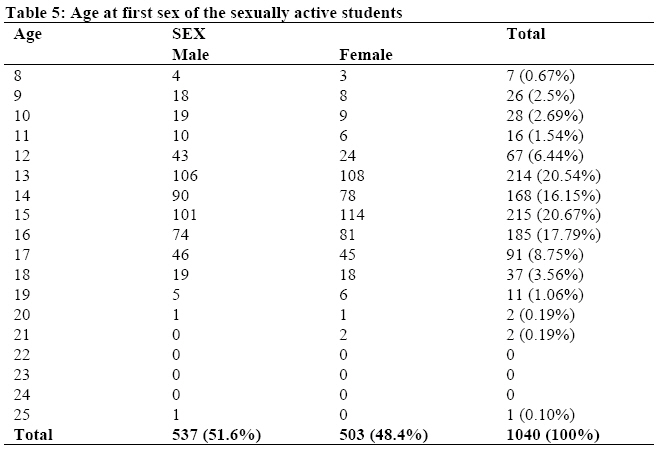
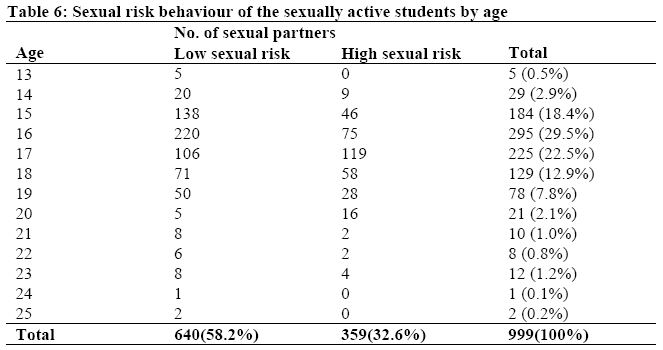
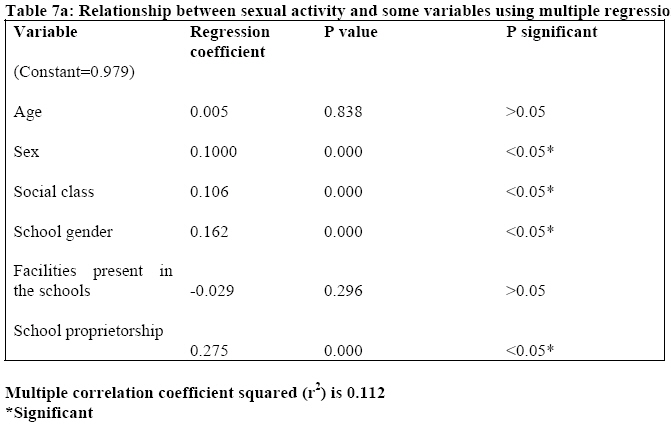
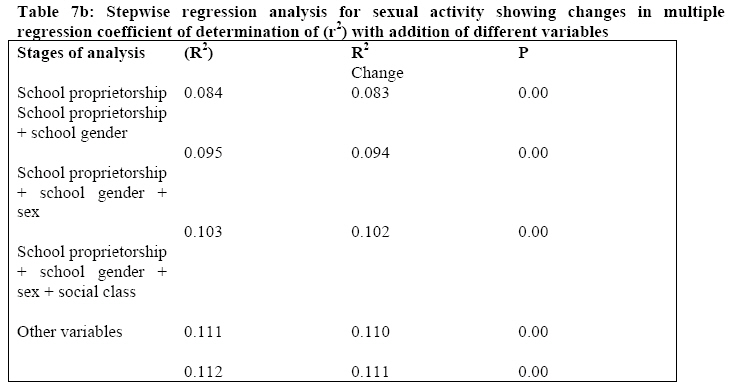
African Journal of Health Sciences, Vol. 15, No. 1-2, Jan-Mar, 2007, pp. 42-49 Prevalence of major HIV- risk related behaviour among SSS3 students in Port Harcourt Metropolis, Nigeria Abiola A. Aomreore and Edward A.D. Alikor* University of Port Harcourt Teaching Hospital, Port Harcourt Code Number: jh08008 SUMMARY The paper intended to find the prevalence of HIV infection risk-related behaviours among third year senior secondary school students in Port Harcourt metropolis. A cross-sectional survey among 1800 third year senior secondary school students randomly selected from thirteen secondary schools in Port Harcourt metropolis was done using two-stage sampling technique. Demographic data and information on the sexual behaviour of each student in the study group was obtained from self-administered structured questionnaire. The prevalence of sexual intercourse was 61.1%. Males were more sexually active than females. Age of first sexual intercourse was 13.2±5.6 years for males and 13.9±4.1 years for females. Of the sexually active students, 32.6% had multiple sexual partners. Sexual activity of the students did not increase with age. The prevalence of Intravenous drug use (IVDU) was found to be 1.4%. The use of intravenous drugs was more among the males (80.8%) than among the females. The prevalence of blood transfusion is 10.3%. Among the sexually active students only 437 (36.9%) used condom. Sex of student, social class and school gender were significant predictors of ever-had sexual activity. The paper concludes that the prevalence of sexual behaviour related to the development of HIV/AIDS amongst the students is high. The need to highlight HIV/AIDS education programmes in the school curriculum of adolescents is discussed. Introduction Two-thirds of the world's total number of people living with HIV resides in sub-Saharan Africa [1,2]. Sixty percent of all AIDS cases and majority of the new infections are seen in 15-24 year olds1. Adolescence is the time during which behavioural changes that transform a child into an adult occur. Adolescents are particularly vulnerable to HIV because the major risk factors of HIV transmission are common and mostly initiated in adolescence [1,3,4]. They are sexually active, generally do not have a stable sexual relationship [1,4,5] and often ignorant of the health risks of their sexual behaviour. They tend to be sensitive and subject to control by peer pressures. Some of the adolescents may be sexually exploited by adults [4,6]. Those who engage in intravenous drug use (IVDU) are even more vulnerable to sex- or injection-related HIV transmission [6]. Adolescents generally find it difficult to reach health facilities where they can discuss questions related to sexual health. Counselling is rarely available and family planning clinics are mostly restricted to married women and couples. Adolescents are usually reluctant to talk to doctors and parents due to embarrassment and fear of possible lack of respect of their confidentiality [1,3,7]. As they are still developing behaviour and experimenting in sexual matters, they can adopt safer practices from the onset. Their attitudes are usually less rigid and with less entrenched taboos, they can be channelled positively towards AIDS education programmes to spread messages on what is safe and what is not. If they are successfully counselled, they can stay free of HIV and form a reservoir of potential healthy parents [1,3,7].In order to have the basis on which to plan health education strategies on HIV control and prevention, the prevalence and pattern of HIV infection risk-related behaviour among adolescents is essential. This study therefore set out to find the prevalence of HIV infection risk-related behaviours among third year senior secondary school students in Port Harcourt metropolis. Materials and Methods The study was conducted in the metropolis Port Harcourt, in the Niger delta region of Nigeria. The subjects were 1,930 third (final) year senior secondary school students from 13 government approved secondary schools. This sample size meets the estimate of 1,500 required to determine a prevalence of sexual intercourse of 29% [8,9] with an absolute precision of 2.25% at 95% confidence. The study was ethically cleared and approved by relevant school authorities. A two-stage stratified sampling method was used to select the thirteen schools. The details of the sampling method have been stated in a previous publication [10]. Pre-tested structured questionnaires were used to collect demographic and medical information as well as information of the sexual behaviour of the study group. The data was analysed using Statistical Package for Social Science (SPSS) for Window 7.5. The descriptive statistics were obtained. Sexual risk status was computed based on number of sexual partners and classified into two categories: low-risk sexual status, consisting of students with only one sexual partner; and high-risk sexual status consisting of students with more than one sexual partner. Results One thousand nine hundred and thirty (1930) students participated in the study. Data from 1800 students were analysed. Information from 130 (6.7%) students who completed the questionnaires wrongly was not included in the analysis. The mean age of the males was 16.59±1.53 years and that of the females was 16.82 ± 1.62 years. Table 1 shows distribution ever-had sexual intercourse of the study group by age and sex. Overall, the prevalence of ever-had sexual intercourse was 61.1%. Males were more sexually active than females with a prevalence of 53.2% compared to 46.2% in females. Nine hundred and seventy four (61%) of the students aged £18 and 126 (65%) of students aged >18 years admitted to be sexually active. Sexual activity of the students did not increase with age. Table 2 shows the prevalence of IVDU to be 1.4%. The use of intravenous drugs was more among the males (80.8%) than among the females (19.2%). None of the students reported the sharing of needles. The prevalence of blood transfusion is 10.3% as shown in Table 3. Majority (62.4%) of the students who had blood transfusion in the past were females. Among the students who claimed to be sexually active, 13.8% admitted having sexual intercourse rarely, 45.3% occasionally, 8.9% frequently, 1.5% had sex daily, while 30.6% did not respond to the question (Table 4). Table 5 shows the age distribution at first sexual intercourse for males and females. One thousand and forty (94.7%) of the 1100 sexually active students could remember their ages at first sexual intercourse. About 0.2% of the students gave ambiguous answers while 4.9% did not answer the question. Most (70%) of the students had first sexual intercourse between 13 and 16 years. Mean age of first sexual intercourse was 13.2±5.6 years for males and 13.9±4.1 years for females. By the time the students were 18 years of age 89.8% of them had been sexually exposed. Six hundred and forty students (58.2%) reported that they had only one sexual partner in their lifetime while 359 (32.6%) had more than one partner. The distribution of sexual risk with age is shown in Table 6. One hundred and one (9.2%) of the sexually active students did not respond to the question. The sexual partners for 765(69.5%) of the sexually active students, were fellow students. One hundred and eighty three (16.6%) had sexual intercourse with much older adults. Eight respondents (0.7%), all boys, admitted that their sexual partners were commercial sexual workers, 18 (1.6%) reported intercourse with their relatives (uncles, cousins and stepfather) while 11.5% (126) did not indicate whom they had sex with. Among the sexually active students only 437 (36.9%) used condom. The results of the multiple and stepwise regression analysis for the sexual activity of the students are presented in Tables 7a and 7b respectively. Table 7a shows that of the entire variables studied sex; social class and school gender were significant predictors of ever-had sexual activity and with other variables accounting for 11.2% of the variation in ever-had sexual activity. Table 7b shows that school proprietorship alone accounted for 8.4% of the variation, school gender and sex of student accounted for 1.1% and 0.8% respectively. Discussion The prevalence of sexual intercourse of 65.8% found in this study is similar to results from a previous study by Judith et al [11] who reported prevalence of 63.5% but lower than the prevalence of up to eighty percent found by other workers in Cameroon and Nigeria reported [12,13]. Other authors in Nigeria [8,9,14] have found lower prevalence of ever-had sexual intercourse in adolescents of 29 to 35%. Younger average age of the study group, smaller sample sizes of many of the other studies and the reluctance of the adolescent to admit pre-marital sex (which will partly depend on the method, and the environment, of administration of the questionnaire) may explain the lower prevalence obtained in these studies. The more adventurous nature of boys compared to girls, often engaging in sexual relationships merely for sexual experience, may explain increased sexual activity than girls as found in this study, which is also similar to finding from previous studies by Meeker et al [12] and Olufunmilayo et al [14]. The low prevalence of intravenous drug use (1.4%) is not surprising as studies by Adelekan [15]and Ogunremi [16] found comparable prevalence of intravenous drug use between 1.2% and 4.9%. Anochie et al [17] did not find any case of IVDU among the students studied in the same locality as the present study. In contrast, higher (35.6%) prevalence of IVDU has been reported in more developed countries [18]. The higher prevalence of IVDU among boys found in this study is similarly to data from previous studies [17,19]. The early initiation of sexual intercourse found in this study is comparable to that reported by Meekers [12](12.6yrs for females, 13.4yrs for males) and Odunjinrin [20] (12.3 years females). Poor economic conditions (especially with respect to the females) and peer influences have been suggested to encourage early sexual initiation amongst adolescents [14,20]. Sexual intercourse with multiple partners as found in this study is similar to the results of previous studies [9,13,14,20]. Among the sexually active students, only 36.9% reported ever-use of condom. This low usage (36.9%) of condom is similar to the findingsby Judith [11] and Olufunmilayo et al [14] who reported 38.9% and 47.2% of ever-use of condom, respectively. It was however, higher (62%) in Meeker’s study [12]. In this study 11.2% of the variation in the ever-had sexual intercourse status was explained by all the independent variables in the multiple regression analysis. It shows that, of all the variables, sex, social class and school gender of the students significantly affect their ever-had sexual intercourse status. This result agrees with the finding by Meeker [12] who found that students from low social economic class were more sexually active. This may suggest that money could be the motivation for the students in the low social class. Conclusion It is concluded that the prevalence of sexual intercourse is high among the students. Sexual intercourse is initiated at an early age and having multiple sexual partners is not uncommon among the adolescents. Sexual intercourse is commoner among the male and students from state schools. The use of condom is uncommon among the study population. There is need to introduce and emphasise school-based HIV/AIDS prevention programme early in the school before the initiation of the HIV risk-related behaviour. The use of condom should be emphasised. The contents of school health HIV/AIDS prevention and control programs should be evaluated at intervals and modified to achieve effective control of HIV. References
© Copyright 2008 - African Forum for Health Sciences The following images related to this document are available:Photo images[jh08008t1.jpg] [jh08008t7a.jpg] [jh08008t6.jpg] [jh08008t3.jpg] [jh08008t7b.jpg] [jh08008t2.jpg] [jh08008t4.jpg] [jh08008t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}