 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Medicine and Biomedical Research, Vol. 3, No. 1, June 2004, pp.81-85 Thyrotoxicosis in Benin City: a study of surgical treatment of 50 patients U Osimea and MN Okobiaa aDepartment of Surgery, College of Medical Sciences,
University of Benin/University of Benin Teaching Hospital, Benin City, Nigeria.
Code Number: jm04012 ABSTRACT Thyrotoxicosis is regarded as uncommon in sub-tropical Africa, although recent reports seem to indicate an increasing frequency of this disease. From January 1986 to April 2001, 50 patients were operated upon for thyrotoxicosis at the University of Benin Teaching Hospital. Forty seven of them were females and three males (ratio 15.7:1). Poor compliance with drug therapy, relapse in symptoms, increase in the size of the goitre and cosmesis were the main indications for surgery. Sub-total thyroidectomy uniformly produced good results from the limited follow-up; few complications were associated with this procedure. The patients generally had good haemoglobin levels > 10g% on admission and no blood transfusion was used in the series during or after surgery. There was no mortality. It is recommended that in sub-tropical Africa, surgery for thyrotoxicosis is a safe, effective and reasonably cheap procedure when compared to other modalities of treatment. Key Words: Goitre, thyrotoxicosis, sub-total thyroidectomy INTRODUCTION Goitre is a common disease throughout the world but the reported incidence of thyrotoxicosis varies considerably among the continents and even among the countries of the same continent. Earlier investigations by Davey and Ogunlesi1, Nwokolo and Ekpechi2, Patel3, Adesola4 and Osime5 reported a low incidence of thyrotoxicosis in sub-tropical Africa. More recently, Morgan6, Obiekwe7, and Osime and Ofili8 have reported an increasing frequency of the disease within the sub-region. In North America, it is known from reports in literature that thyrotoxicosis occurs in almost equal frequency between the African-Americans and white Americans. The purpose of this retrospective study is to report our surgical experience in 50 patients with thyrotoxicosis over a period of 15 years so as to highlight any peculiarities and similarities with others in the relatively more advanced countries having modern day technology.
PATIENTS AND METHODS This is a retrospective study in the surgical department of the University of Benin Teaching Hospital from August 1986 to April 2001 in which records were examined from the outpatient department, surgical wards and the theatre records. Relevant data were retrieved on the age of patients, sex, clinical features of thyrotoxicosis, investigations, diagnosis, pre-operative preparation of patients, type of surgery, weight of excised goitre, histology, complications of surgery, associated medical diseases and follow-up.
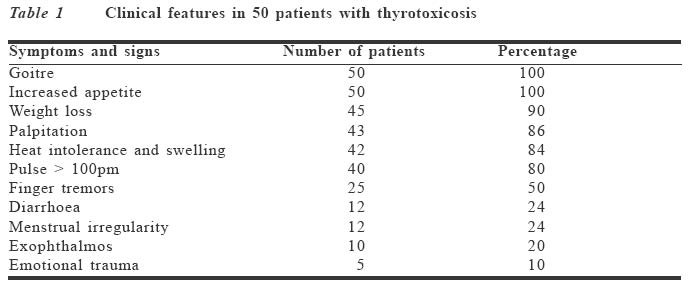
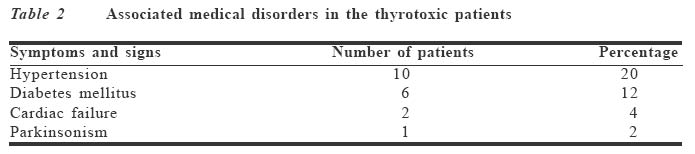
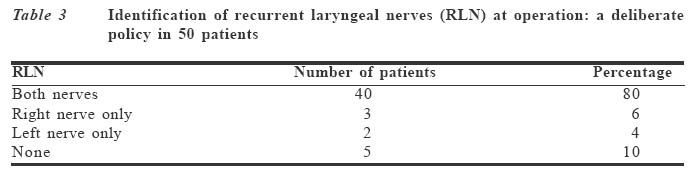
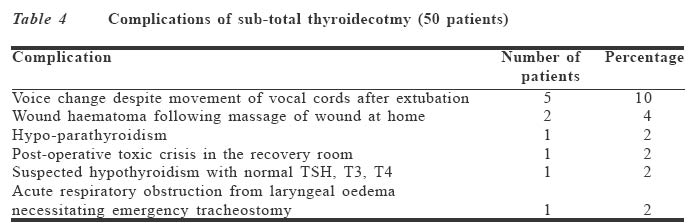
RESULTS A total of 367 patients with thyroid disease were admitted for surgery during the period. Of these, 50 patients (13.6%) had thyrotoxi-cosis, comprising 47 females and three males. Their ages ranged from 19 to 74 years (mean 39 years, SD 16.52 years). Patients with primary thyrotoxicosis had an age range of 19 to 48 years with a mean of 32 years (SD. 10.03 years) while the range for secondary toxic goitre was from 43 to 74 years (mean 60 years, SD 11.45 years). The clinical features were typical of thyrotoxicosis, as indicated in Table 1. Table 2 shows diseases that were associated with toxic goiter. Figure 1 shows a patient with primary thyrotoxicosis and exophthalmos. The main specific investigations were limited to thyroid stimulating hormone (TSH), tri-iodotyronine (T3) and thyroxine (T4) serum estimation. Other relevant investigations were conducted as shown in Table 3. The majority of patients had reasonable haemoglobin > 10g%. All the patients were rendered euthyroid, using carbimazole, propanalol, L-thyroxine and diazepam and continued to take the drugs until surgery. Only propanalol was continued for five days after surgery. Pre-operative Lugol's iodine was not used in this series due to non-availability of the drug. The standard operation that was carried out was sub-total thyroidectomy aiming at a thyroid remnant of 3-4g or 3 x 2 x 1cm10-12 on each side, i.e., one third of a normal thyroid gland. It was our policy to identify as much as possible both the recurrent laryngeal nerves (Table 3) and the parathyroids. There was no occasion in which it was necessary to divide the strap muscles even with some large goitres. The need for blood transfusion did not arise and consequently no blood was given during the period of study. Although there was no mortality, the complications following sub-total thyroidectomy are enumerated in Table 4. The most serious complication was a case of hypo-parathyroidism that occurred in one of four siblings comprising mother, two daughters and a son in the series. The female patient recovered after 12 months of treatment. The histology reports on the specimens were in support of thyrotoxicosis with no evidence of malignancy. The weights of goitre resected varied from 50 to 700g with an average of 143g. The follow-up period was satisfactory for the first three years; all patients were seen at six weeks after surgery, then six months later, and thereafter at yearly intervals. By the 5th year barely 20% kept their appointments.
DISCUSSION In a publication from this centre in 19845, seven patients out of 150 (4.7%) were found to have thyrotoxicosis over a seven-year period, which was similar to reports from other parts of sub-tropical Africa.1-4 However, our present study and a more recent publication7 from Enugu indicate an increasing frequency (13.5% and 16.5% respectively). Thyrotoxicosis is a disabling and distre-ssing disease due to the hypercatabolism and cardiovascular complications associated with the disease particularly when it is not recognised in the sub-tropical region either because of lack of medical specialists or lack of investigation. However, in a modern setup, thyrotoxicosis is not a difficult diagnosis to make, as most of our patients presented with the classical features of the disease. Also, all our patients in this study had at least serum TSH, T3, T4 estimations, which in all cases corroborated the diagnosis of thyrotoxicosis. Patients were made euthyroid on a combination of carbimazole (10mg 8 hourly), propanalol (40mg 12 hourly) and L-thyroxine (0.1mg daily). Good indicators of a positive response to therapy were weight gain, disappearance of heat intolerance, return of pulse to normal and disappearance of finger tremors. The main indications for surgery were large goitres causing compression symptoms, failure of compliance with drug therapy, frequent relapses on medical treatment and cosmesis. There is no consensus on the exact amount of thyroid remnant that is to be left behind in sub-total thyroidectomy. Even with the same surgeon the amount of thyroid remnant may vary from one patient to the other. There is as yet no general formula that is applicable to all patients on how much of the goitre is to be excised. However, there is enough information from literature to suggest that it is better to err on the side of removing too much than too little.9-11 Our results show that leaving a thyroid remnant of 3-4g or 3 x 2 x 1cm on each side is associated with good results, and this is in keeping with the reports of others. 10,.11 The treatment of thyrotoxicosis varied greatly from one area to the other depending on the facilities and expertise available. Medical treatment, radio-iodine therapy and surgery are the main tools to manage thyrotoxicosis, and each has its own advantages and disadvantages. Radio-iodine therapy is outside the reach of most patients in the sub-tropical region of Africa and with medical treatment there is a high 50% incidence of relapse, which often drives the African patient to try alternative traditional medicine with disastrous results. The results of surgery in our study have been good with no mortality and few compli-cations (Table 4). The most serious complication in our experience was a young patient aged 22 years who developed hypoparathyroidism on the third post-operative day and needed treatment for 12 months before returning to normal. This patient had a low (8.5g%) pre-operative level of serum calcium. It is possible that with a longer follow-up, other complications such as recurrent thyroto-xicosis or hypothyroidism might show up. However, published reports7-9 show that recurrent thyrotoxicosis tends to occur within 18 months of surgery. The suspected case of hypothyroidism with normal TSH, T3 and T4 did not require treatment during six months of observation before the patient was lost to follow-up. The voice changes reported in five patients improved with time. During the early period of this study, there was no ENT surgeon in the hospital to perform indirect laryngos-copy, and consequently the status of the vocal cords was not always known. However, the anesthetist had assisted after extubation in noting the movement of the vocal cords. It is interesting to note that in all five patients with voice changes, the anesthetist had observed that the vocal cords moved. Taylor and Painter9 had observed that voice changes after partial or sub-total thyroidectomy may be unrelated to recurrent laryngeal nerve damage. It is of interest to note that four members of the same family, comprising the mother (52 years), two daughters (25 and 27 years) and a son (23 years) were in this series, which shows that obviously thyrotoxicosis can have a strong familial trait. We observed that most patients with goitre have a reasonable haemoglobin level > 10g% and the blood loss varied from 25 to 175ml with an average of 100ml. There was no cause to transfuse our patients during or after surgery.
CONCLUSION This retrospective study would appear to show an increasing frequency of thyrotoxicosis in the sub-tropical Africa, compared to about 50 years ago. Sub-total thyroidectomy after patients have been made euthyroid is safe and effective with few complications and is recommended as the treatment of choice for thyrotoxicosis in sub-tropical Africa.
ACKNOWLEDGEMENT We are grateful to the consultants and resident doctors of the Department of Surgery who participated in the management of these patients. References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm04012t4.jpg] [jm04012t2.jpg] [jm04012t1.jpg] [jm04012t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}