 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Medicine and Biomedical Research, Vol. 4, No. 1, June 2005, pp. 71-77 Vaccination default rates among children attending a static immunization clinic in Benin City, Nigeria AN Onyiriuka Department of Child Health, College of Medical Sciences, University of Benin, Benin City, Nigeria.
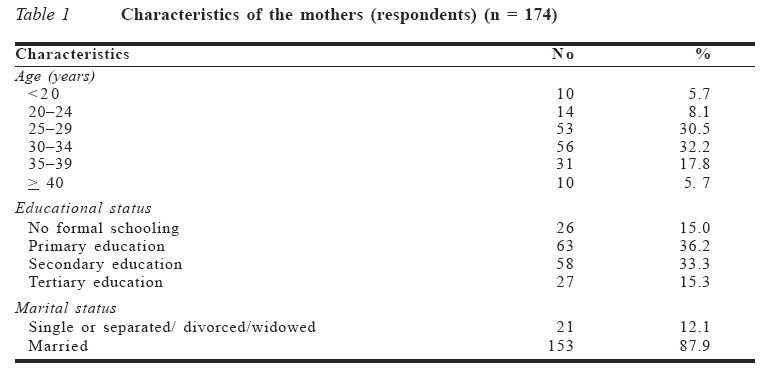
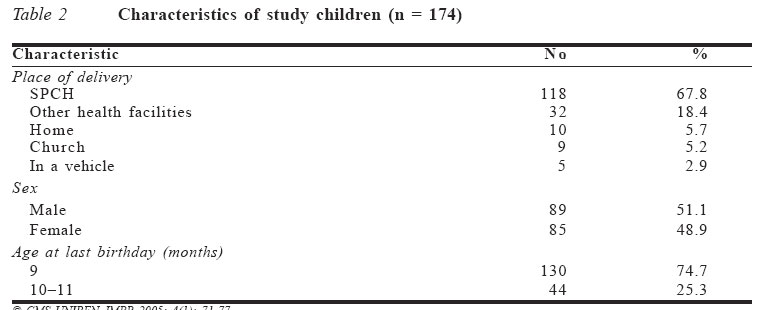
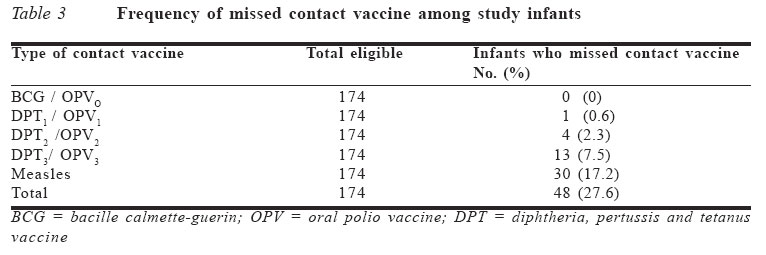
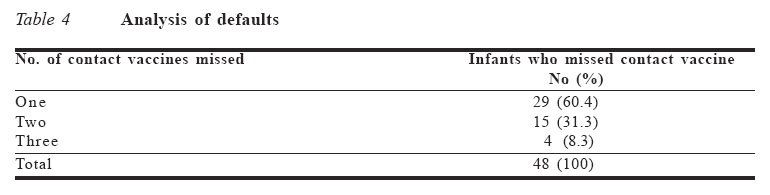
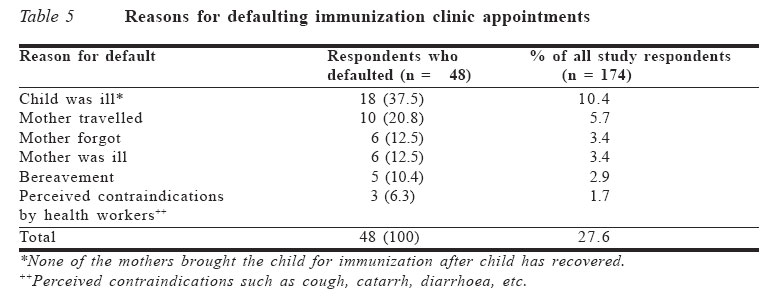
Code Number: jm05010 ABSTRACT Immunization coverage among infants in Nigeria continues to be low despite availability of effective vaccines and accessibility of immunization clinics in urban areas. This study was conducted to determine the vaccination default rate and vaccine schedule that is most frequently defaulted. It also documented reasons for the defaults and suggested ways of minimising them. The immunization status of 174 children aged 9-11 months were determined by interviewing mothers regarding their children's immunization histories. Each child's immunization card was subsequently reviewed for confirmation. Overall default rate for the entire recommended series of vaccines was 26.7%. Measles vaccine was the most frequently defaulted. The commonest reason given by respondent mothers for defaulting immunization clinic appointments was the child's ill-health (37.5% of all cases). Immunization clinic appointment default rate is still high in Benin City, with measles vaccine being the most frequently defaulted. We therefore suggest ways of minimising vaccination clinic appointment defaults. KEY WORDS: Childhood, vaccination, default, Nigeria INTRODUCTION The induction of an immune response to infectious diseases by vaccination has become a widely applied and cost-effective public health intervention.1,2 For immuni-zation to be effective as a long-term global childhood disease control strategy, it is essential for parents to continue to present their children for vaccination. The 1990s witnessed declining vaccination coverage rates.3 For instance, in Nigeria, immunization coverage of 80% was achieved in 1990, but by 1993 the coverage has fallen to 30%.4 In Nigeria, routine immunization against the childhood vaccine preventable diseases usually requires the child to make five visits to a static immunization clinic. At each visit the mother is given appointment dates (written on the child's registration card) for the next vaccination. Despite this approach, non-compliance with immunization schedules by mothers have been reported to be one of the contributory factors to low immunization coverage in Nigeria.4-5 Several studies on immunization coverage have relied on samples from clinic-based records.6-8 Such studies may give biased estimate of immunization levels in the general population. Despite this shortcoming, data collected from clinic-based records can give a substantial insight into the level of immunization coverage and the factors that influence it. This study sought to determine vaccination default rate, the vaccination schedule that is most frequently defaulted and to document reasons for the defaults. It also suggested ways of minimising these defaults. PATIENTS AND METHODS This cross-sectional study was conducted in a static immunization centre located at the St Phelomena Catholic Hospital (SPCH), Benin City. It is a large mission hospital established 62 years ago and is located in the centre of Benin City, the Edo State capital. The immunization clinic is well patronized because of its central location, good access road (no flooding during the rainy season) and, above all, regular availability of vaccines. The vaccination sessions begin at a scheduled time and close when all the children in attendance have been vaccinated. Waiting time by mothers is usually short (<30 minutes). Mothers pay a token fee to cover the cost of consumables such as syringes, needles, cotton wool and methylated spirit used in administering the injectable vaccines. During each visit, mothers are given appoint-ment dates (written in the child's registration card and communicated to them verbally) for the child's next vaccination. Vitamin A is also administered during these vaccination sessions. Infants discovered to have any medical problem are referred to the consultant paediatrician for evaluation and treatment. Thus, the mothers have a positive perception of the quality of vaccination services offered at SPCH. The study population included all mothers attending this static immunization clinic, who had children aged 9-11 months on the day of the interview. Different vaccines are offered on different days in this study facility to minimise vaccine wastage, namely, BCG/OPVO on Thursdays; DPT / OPV on Mondays, Tuesdays and Fridays. Only measles vaccine is offered on Wednesdays. Children aged 9-11 months were chosen for the study, to allow for a review of the child's immunization history from birth to the age of nine months, when s/he should have ideally completed all the recommended series of primary immuni-zation based on the current immunization schedule for infants in Nigeria. The survey was conducted every Wednesday over a period of three months, September 1 to November 30, 2003. The choice of Wednesday, the only day measles vaccine is offered, was to enable us to reach children aged 9-11 months who constituted the study population. In Nigeria, measles vaccine is usually given at about the age of nine months. The interview included questions on maternal age, education and marital status. Other information obtained included place of child's delivery, date of birth, perception of quality of vaccination services and, where applicable, reasons for failure to complete immunization. Each mother was also asked whether her child(ren) had been refused immunization within the 12 months preceding the interview day and, if so, to state the primary reason for the refusal. The child's immunization card was subsequently examined to obtain information on the number of visits made, vaccines received with dates, and the appointment dates that were given. The criteria used for age-appropriate vaccination allowed for a 28-day grace period for the receipt of each vaccination, and a child who had received all indicated vaccines within 28 days of becoming age-eligible was considered to be age-appropriately vaccinated. A "missed opportunity" is when a child who needed an immunization had contact with the health service but was not given the vaccination. A contact vaccine refers to any of the five sets of vaccines - BCG/OPVO, DPT1/OPV1, DPT2/OPV2, DPT3/OPV3 and measles - administered at a particular age and contact in the immunization schedule. Statistical analysis involved calculation of ratios, percentages, means and confidence intervals. RESULTS A total of 174 eligible mothers were interviewed. All the children were brought to the vaccination sessions by their mothers (none by their fathers). The mean age (SD) of eligible mothers interviewed was 26.3 years (95% CI = 26.1-26.5) with a range of 18 to 42 years. The mean age at which the respondent mothers had their first child was 23.1 years (95% CI = 22.9-23.2) with a range of 20 to 31 years. Further details are shown in Table 1. Age-appropriate immunization Since 174 infants were studied, the total contact vaccine doses (at five contact vaccine doses per child) was 174 x 5 = 870. Only 51.7% (450/870) of contact vaccine doses were given at the correct time and interval (95% CI = 0.516-0.518). The mean number of immunization shots received by the study children in the series was seven out of a maximum of nine. Reliability of immunization histories given by mothers Of the 174 respondents, 21 (12.1%) admitted to having missed immunization appointment for their present child(ren), but when their child(ren)'s immunization cards were checked, 48 (27.6%) were found to have defaulted clinic appointments. As shown in Table 1, most (62 .6%) of the respondents (mothers) were in the 25-34 years age group. Only 5.2% and 5.7% of the respondents were aged <20 years and >40 years respectively. One hundred and twenty one (69.5%) respondents had either primary or secondary education. Most (87.9%) of the respondents were married. As shown in Table 2, majority (86.2%) of the study children were delivered in health facilities, while the remaining 13.8% were delivered at home, at the church or in a vehicle. One hundred and thirty (74.7%) of the 174 study children aged 9-11 months were aged nine months, while the remaining 44 (25.3%) were aged 10-11 months. The sex ratio was 1.05:1 in favour of the males. One hundred and twenty six (72.4%) of the infants completed the entire immunization schedule recommended for the first 11 months of life (Table 3). Immunization rates were higher initially but dropped for subsequent vaccines in the series. Hence, the vaccine most frequently defaulted was measles vaccine (17.2%), followed by DPT3/OPV3 (7.5%). As shown in Table 4, 48 (27.6%) of the 174 study infants missed one, two or three contact vaccines. Majority (62.5%) of them missed only one contact vaccine. Only 8.3% of them missed three contact vaccines. Child's illness (37.5%) was the commonest reason for missing an immunization appointment (Table 5). DISCUSSION The overall rate of default for the entire series of vaccinations in this study was 27.6%. Although high, it is lower than the 37.2% reported in Ilorin.8 This may be explained by the fact that a greater proportion of respondent mothers in this study had tertiary education, compared to the Ilorin study.8 It is also possible that the quality of vaccination services offered in this study facility was better than that offered in the study facility at Ilorin.8 This study, however, did not include data on the quality of vaccination services in the study facility. The high default rate observed in the study may lead to eventual dropout if the trend is not urgently checked. One way to do this, is by ensuring that all clinics providing immunization educate mothers about the importance of timely childhood immuni-zation and the need to complete the entire schedule of vaccination to ensure full protection against the six childhood vaccine preventable diseases. Although majority of infants of defaulting mothers missed only one contact vaccine, it must be realised that the timing and combination of vaccines are very important in obtaining best results and in avoiding unscheduled visits to the immuni-zation clinics.4,9,10 Unscheduled visits may increase the total cost of transportation, thereby dampening the enthusiasm of mothers to attend vaccination clinics. In contrast to the Ilorin study in which BCG/OPVO was the most frequently defaulted vaccine, no case of default for BCG/OPVO vaccine was recorded in this study. This may be explained by the fact that majority (66.5%) of the study children were delivered at SPCH, which provided them the opportunity of being vaccinated with BCG/OPVO at birth before discharge from hospital. It is also possible that the joy and sense of fulfilment that follow the arrival of a newborn infant in a family, coupled with the short interval between the delivery of the infant and administration of B CG/OPV0, reduced the chances that mothers would forget immunization (BCG/OPV0) clinic appointment, as this was one of the reasons given by mothers for vaccine defaults. In this study, measles vaccine was the most frequently defaulted. Other investigators have reported a similar finding.5,11 This finding may be explained by the relatively long time interval (35.5 weeks) in clinic appointment between the third dose of DPT (at 14 weeks) and when the child is due for measles vaccine at the age of nine months. This may have made mothers to forget immunization clinic appointment dates. To address this problem, mothers should be encouraged to attend monthly growth monitoring clinics, which should be incorporated into the vaccination services. Administration of prophylactic vitamin A to children at nine months along with the measles vaccine may serve as an inducement for mothers to bring their children for measles vaccine. In addition, health workers should encourage mothers to keep their husbands informed of the new appointment dates after each immunization visit. The usefulness of this approach is supported by the results of a Ghanaian study, which showed that children are more likely to complete the immunization schedule promptly if their fathers are involved in any aspect of the immunization programme.12 Once any mother defaults on any of the contact vaccines, defaulter tracing in the form of home visit should be instituted. This approach will help strengthen the delivery of static immunization services. In this study, the commonest reason given by respondents for defaulting on child's immunization was child's illness, whereas mother's forgetfulness was the commonest reason reported by Musa in Ilorin.8 In that study, only 10.4% of defaults was due to the child's illness. However, these mothers did not bring their children for immunization after they had recovered from the illness, thus suggesting that they may have had the misconception that a minor illness is an absolute contraindication to vaccination. Educating mothers that minor ailments such as mild fever, cough, upper respiratory tract infection, diarrhoea, etc, are not contrain-dications to vaccination will correct this misconception. All the respondents confirmed that their appointment dates were written on their home-based cards. Furthermore, in 95% of cases the health worker told the mother the date of the next visit. This is commendable of the health workers. This practice is in consonance with the recommendation that immunization clinic appointments should be written in the child's card as well as communicated to the mother by the health worker.13 In consonance with a previous report,8 none of the mothers mentioned side effect of previous vaccination as a reason for defaulting clinic appointments. This is a re-assurance of the safety of vaccines and a confirmation of the technical competence of the vaccinators in this clinic. Poor staff attitude, poor vaccination services and non-availability of vaccines on the appointed dates were not mentioned as reasons for defaults. Musa in his study reported similar findings.8 On the other hand, some investigators have reported poor staff attitude and poor quality vaccination services as reasons for defaults in some immunization clinics.14-16 In 6.3% of cases, vaccination defaults were attributed to health workers' misconception about contraindications to vaccination, which may lead to missed opportunity. The role of missed opportunity in vaccine default has been reported by other investigators.6,16,17 This implies that more efforts are needed to ensure that missed opportunities for immunization are minimized through in-service training of health workers to correct misconception about contraindications to vaccination. In contrast to other reports11,16 that male gender is a significant predictor of delayed immunization, no gender difference was found in this study. Other investigators20,21 did not also find any gender difference in immunization status of their study children. In this study, many mothers gave inaccurate immunization histories. Other investigators in Nigeria,5,8 USA16 and Australia22 have reported similar observations concerning accuracy of immunization histories. We therefore recommended that doctors should always endeavour to review children's immunization documents during hospitali-sation to obtain more accurate immunization histories. ACKNOWLEDGEMENT I am sincerely grateful to all staff at the immunization clinic of SPCH for pain-stakingly documenting the immunization dates and records used in this study. The manuscript was typed by Miss Blesyn Efoghe. References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm05010t4.jpg] [jm05010t3.jpg] [jm05010t2.jpg] [jm05010t5.jpg] [jm05010t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}