 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Medicine and Biomedical Research, Vol. 5, No. 1, June 2006, pp. 24-28 Prevalence of Undiagnosed Diabetes Mellitus Among Dental Patients in Edo State, Nigeria Ojehanon P. I.1 and O. Akhionbare 2 1Dr. P. I. Ojehanon, Department Of Periodontics, School
Of Dentistry, College Of Medical Sciences, University Of Benin, Benin City,
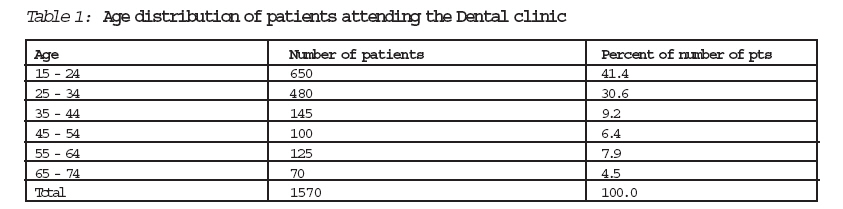
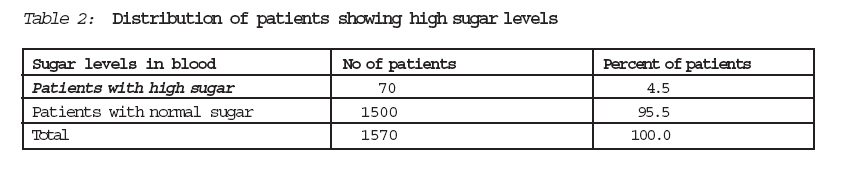
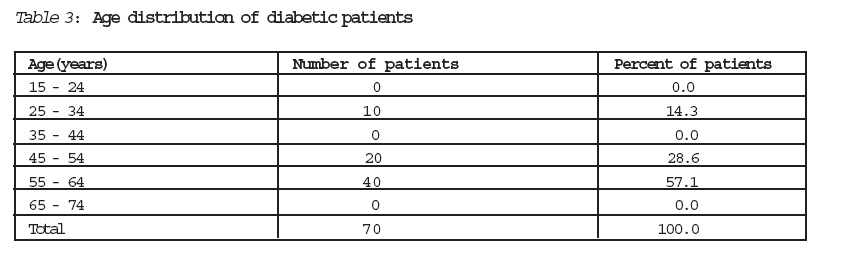
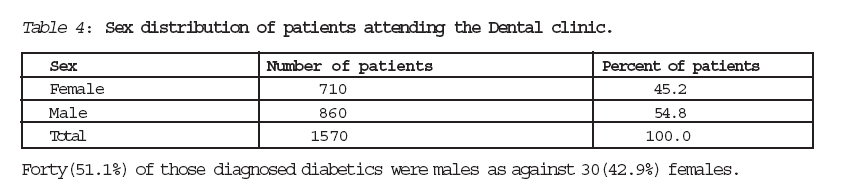
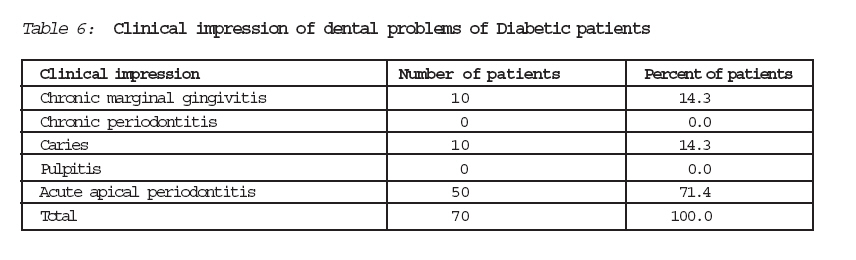
Nigeria. Correspondence: Dr. P. I. Ojehanon, Department Of Periodontics, School Of Dentistry, College Of Medical Sciences, University Of Benin, Benin City, Nigeria. Code Number: jm06005 ABSTRACT Diabetes mellitus is a common condition which can lead to medical complications and can have an adverse effect on oral health and health-care. It has been reported that individuals with poor sugar control loose more teeth, have increased incidence of dental anomalies and diseases including periodontitis, dental caries and candida infections. The study population of 1570 patients attending the dental clinics at the University of Benin Teaching Hospital Benin city, aged 15 - 75 years were screened for urinary glucose using the clinistix dipstick method initially followed by fasting blood sugar. Over four percent (4.5%) of all the patients showed high glucose level in blood with 42.9% females and 57.1% males. 28.6% of these patients showing high glucose levels were aged 45 to 54years while 57.1% were between 55 and 64years. About 4.5% of patients were unaware of their diabetic status and its effect on oral structures. Screening for sugar in urine should be mandatory for all dental patients. All those with sugar in urine should be further screened and referred to the physician if blood levels are high. Health talks about the effect of diabetic condition on the health of oral structures should be given at patients first visit to the dental clinics. All the patients showing high sugar levels should be treated with the care the condition deserves. KEY WORDS: Diabetes mellitus, urine, sugar level INTRODUCTION Systemic diseases and hormonal changes have been implicated as complicating factors for periodontal diseases1. Gingivitis and period-ontitis are sometimes the first evidence that a patient has diabetes2. Given that diabetes may be present for a number of years before it is diagnosed, Dentists may be the first health professional to detect patients with diabetes2. Gingivitis is initiated often by microbial plaque deposits on the dentogingival interface but progression to periodontitis is modified by several environmental, behavioural, biological and health care variables2,3. Periodontal disease is a common chronic inflammatory disease and an important factor for tooth loss4. Vascular changes, neutrophil dysfuntion, altered collagen synthesis and genetic predisposition observed in diabetes may contribute to periodontitis5,6. Diabetes has been associated with changes in diet and subsistence patterns. Bone and teeth reflect the health of individuals who undergo a change in subsistence pattern7,8. Diabetes is a common condition which can lead to medical complications and can have an adverse effect on oral health and healthcare3,9. It has been reported that individuals with poor blood sugar control loose more teeth, have increased incidence of dental anomalies and diseases including caries and candida infections10,11. When blood sugar level is poorly controlled, the resultant high levels in oral fluids may help microrganisms grow and set the stage for periodontal diseases1,12. The glycaemic status of diabetic patients affects the periodontal probing depth, salivary PH, buffering capacity and peroxidase activity12,13. The objectives of this study are 1. to determine the proportion of dental patients who were diabetic but unaware. 2. To evaluate any common clinical presentation among these diabetic patients and their response to instituted treatment modalities. This study was carried out at the University of Benin Teaching Hospital Dental centre located at the university Benin main campus, Benin city which is largely dominated by students (undergraduate and postgraduate), staff and some patients from surrounding environments. MATERIALS AND METHOD All the patients aged between 15 and 75 years attending the dental centre for the first time at the period of study (2003 and 2004) and were not known diabetes were included in this study. Both sexes were represented as determined by attendance for the period. All the patients had their urine screened for sugar and protein using the clinistix dipstick method. The urine examination was done before clinical oral examination. All those patients who showed sugar in urine were sent for fasting blood sugar. Fasting blood sugar levels of 126mg/dl and above was considered diabetic. Diagnosis of patients dental condition was made with appropriate referral to areas for attention to presenting dental complaint. Treatment procedures given were noted and response to such treatment procedures was monitored through review visits. All the patients showing high sugar levels were referred for further management by the physician. At the dental clinic, record notes of patients that showed high sugar levels were also marked/ indicated to act as a guide to the Dental surgeon managing the dental complaint. Note was made of the patients occupation, educational status, any known illness and any drug the patient was on. All data collected were reviewed and stored in a personal computer. Variables were recorded in tabular forms. Analysis of data was done using frequencies and percentages. RESULTS Forty one point four percent (41.4%) of the total number of patients examined at the dental centre were within age 15-24yrs 4.5% were within age 65-74yrs. Four point five (4.5%) of the total number of patients examined showed fasting blood sugar levels of 126mg/dl and above while 95.5% did not. Of the 70 patients showing high sugar levels, 40(57.1%) were aged 55-64 years while 28.6% were aged 45-54 years. Assessment of patients dental complaints showed that of the diabetic patients, 50(71.4%) had a diagnosis of acute apical periodontitis made while diagnosis of chronic marginal gingivitis and caries were made for 14.3% each. DISCUSSION The determination of sugar in urine was done with clinistix dipstick used according to manufacturers' instructions14,15. This was a prelude to a more confirmatory test of fasting blood sugar carried out. It is one of the methods for detection of diabetes16. The clinistix method is not necessarily useful for quantification of sugar contents so it is not advisable to base diagnosis and therapy on clinistix findings16,17. More patients (41.1%) between the ages of 15yrs and 24yrs were in attendance while 70(4.5%) were in ages between 65yrs and 74yrs. The institution of study is located within the university campus which is largely dominated by the age group of 15-24yrs. It is likely that the level of education and therefore awareness on dental issues is more in this age group2,18 . The older group may have less reasons for dental attention since it has been reported that this age group border less about aesthetics, they are affected less by caries and more by periodontal diseases19,20. Seventy (4.5%) of the total number of patients seen were diabetic. This number is higher than the reported prevalence of 2.7% of undiagnosed diabetes in American hispanics14. This higher figure may be related to dietary pattern and availability of screening. The reported figure of 2.7% was among Hispanic whites while this study was in African blacks14. The difference in prevalence may also be related to screening method used. The study that reported 2.7% prevalence rate also used the fasting plasma glucose method. Of the 70 patients showing high sugar levels, 40(57.1%) were within age group 55-64 yrs and this figure represent 32% of total number of pts in the age group. This age group has been reported to have prevalence of 8.9% which is similar to other findings14,15. It has been suggested that in this age group more (866) males were in attendance at the time of study which may be the reason why it appears as if more males (40) were diabetic compared to females (30). Otherwise there is no difference in sex distribution of undiagnosed diabetic. CONCLUSIONS This study shows that some (4.5%) of the patients attending the dental clinic were diabetic even though they were unaware of their diabetic status at the time of visit to the clinic. It would appear that the middle aged and younger Dental patients are more affected with no sex predilection. RECOMMENDATIONS There is the need for routine urine examina-tion for all patients visiting the Dental clinics. Those patients showing sugar in urine should be sent for fasting blood sugar or any other confirmatory test for diabetes. Diabetic patients should have oral and dental examinations more often. Health education about systemic conditions particularly diabetes should be carried out for new dental patients. They should be advised to go for screening for diabetes and other medical conditions. Table 1, Table 2, Table 3, Table 4, Table 5, Table 6 References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm06005t1.jpg] [jm06005t2.jpg] [jm06005t6.jpg] [jm06005t4.jpg] [jm06005t5.jpg] [jm06005t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}