 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
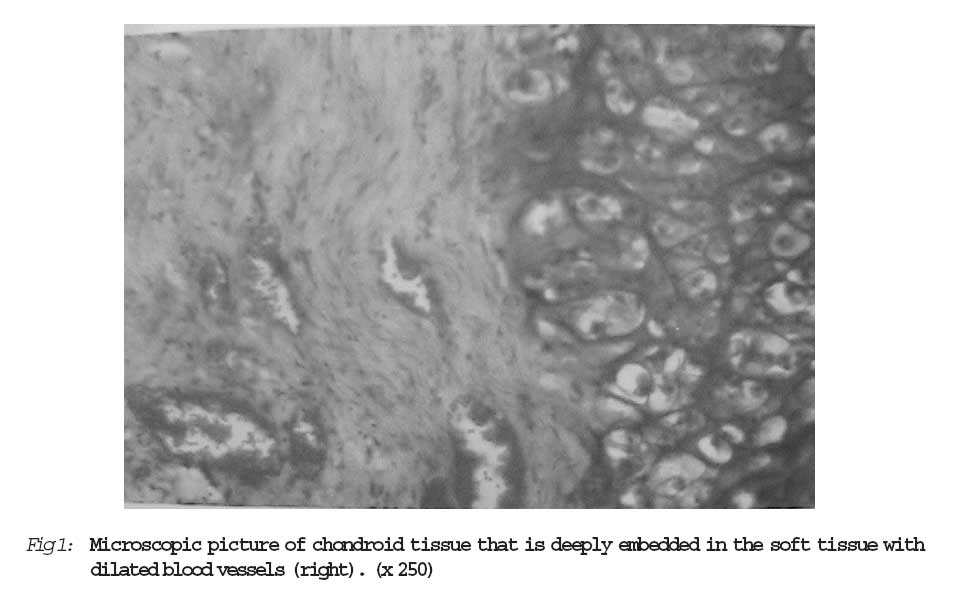
Journal of Medicine and Biomedical Research, Vol. 5, No. 2, December 2006, pp. 18-21 Recurrent Extra Skeletal Soft Tissue Chondroma in a Black African Female: Report of a Case and Review of Literature aEkanem, Victor James bAdeoye I. I. cMarchie, T. T. aDepartment of Pathology, College of Medical Sciences, University of Benin, Benin City, Edo State, Nigeria Correspondence to: Ekanem, Victor James E-mail: vekanem2000@yahoo.com Code Number: jm06014 ABSTRACT Extraskeletal chondroma occurring in the gluteal region is a very rare tumour. Its presence in an abnormal side can pose a diagnostic dilemma. The common sites are usually the hands and feet. We present the clinical and histological feature of a huge recurrent extraskeletal chondroma occurring in the buttocks of an African female. A 22year old athlete living the Niger delta region of Nigeria presented with a recurrent swelling embedded in the soft tissue of the right buttocks which lasted for a period of 1 year. The initial lesion was for a period of 3 years. Histological examination showed an encapsulated lesion composed of matured hyaline cartilage without atypia. Appropriate initial diagnosis is necessary for proper treatment to be instituted to avoid recurrence, since a second surgery maybe difficult particularly in an African where treatment of diseases are influenced by taboos and cultural believes to a large extent. Keywords: Chondroma, buttocks. Introduction Cartilaginous tumors occurring at extra skeletal site are rare lesions. Only very few cases has been reported in literature. Most of the cases occur in the distal phalanges, the toes and fingers1-3. Only very few cases occurring on the trunk have been reported. The age of occurrence so far reported spans from 30 years to 60 years4. Most of the reported cases are in Caucasians and the Mongols. To the best of our knowledge there is no reported case of extraskeletal chondroma in Africans. Here we present the case of a 22 year - old female who presented at our clinic with a one year history of recurrent swelling in the soft tissue of the right buttocks. The initial swelling lasted for 3 years before excision. Case Report A 22 year old female athlete, born and resident in the Niger Delta region of Nigeria presented at our out patients clinic with a mass in the right buttock. The mass was painless and increased in size up to the size of a table tennis ball. Similar mass at the same location and which lasted for a period of 3years before excision biopsy was done was reported histologically to be chondroma. The recurrence occurred a year later and grew rapidly to almost the same size but became painful. There was no associated weight loss, paraesthesia or bone pain in the right limb. Similar swelling has never been recorded in her family. She could not remember any history of trauma. Physical examination reveal a normal healthy looking female except for the swelling in the right buttock occupying the outer upper quadrant of the right gluteal region. The outer surface appears lobulated and there was a transverse scar parallel to the right iliac crest. The scar was most probably due to the previous excisional biopsy performed a year earlier. The mass was slightly tender, firm and measured approximately 10cm x 8cm x 8cm. The overlying skin was free and it was not attached to the underlying bone. These findings were collaborated by x-ray report of a soft tissue swelling that was not attached to the underlying bone. Microscopic examination of biopsy taken from multiple sides showed aggregate of matured hyaline cartilage with variable sized chondrocytic lacunae arranged in lobular pattern and surrounded by a thin rim of capsule. The diagnosis was that of extraskeletal chondroma. Our patient refused a repeat surgery for fear of recurrence and her believe in taboo and native medication. Discussion Chondromas are made up of well differen-tiated cartilage sometimes mixed with a little osteod following calcification. Its occurrence in soft tissue is uncommon, though there have been reported cases in the joints of the hand, foot and knee5. Rare sites such as fallopian tube6, Parotid gland7 and upper arm8 have also been reported. It may be difficult to recognize some of them radiological except for those ones that are calcified. There is usually no attachment to the underlying bone but may be associated with tendon, tendon sheath or joint capsule. Most of the tumors are usually solitary just as it was seen in our patient. However Dellon and associates have reported bilateral chondromas occurring in left and right fingers in association with renal failure9. The age of our patient was 22 years. This falls below most of those reported in literature which falls between 30 and 60years4. However one case was reported in a 10 year old child10. Though many of the reported cases of Extra skeletal chondroma have evidence of calcification our case lack this feature hence radiologically it presented as a soft tissue swelling. The size of the tumour in our patient was approximately 10cm x 8cm x 8cm. This was determined clinically on physical exami-nation. The exact size of the tumour could not be measured as excision biopsy was not done since the patient refused a repeat surgery. This size is however larger than other reported cases that are usually less than 4cm in diameter4,9. It is possible that the location of the tumour in the loose gluteal region could have contributed to the rapid increase in size and the large size of the tumour. Though CT scan and MRI would have been helpful in determining the exact localization and size of the tumour and its relationship to the adjacent bone this was not possible as these facilities are currently not available in our centre. The microscopic picture of the lesion in our patient showed well formed hyaline cartilage without any area of blast formation or calcification (Fig 1). A report has shown that in one third of the cases there is blast formation11. Most of the tumours are usually made of hyaline cartilage often associated with areas of calcification. Other features that can be seen include, Xantoma like feature and granuloma-like proliferations4. A well differentiated chondrosarcoma is a good differential in our patient especially as we could not examine sections from deeper areas of the tumour. A well differentiated chondrosarcoma usually shows features of abnormal mitoses and necrosis which was lacking in the sections we examined. Other differentials include periosteal chondroma and extraskeletal myxoid chondrosarcoma. The tissue of origin of this tumour is still uncertain though many suggestions have been given. One of the suggestions considered the fact that the site is far from synovium or periosteum and as such could have been a metaplastic change12 while another thinks that it has a synovial origin13. Another author suggested that it might have arisen from the subcoelomic mesenchyme of fallopian tube in their own case6. The usual treatment for Extraskeletal chondroma is a wide excision to prevent recurrence. It was difficult to convince our patient to undergo a second surgery for the same tumour that was excised barely a year before her presentation at our clinic. This stem from her believe that the tumour was of spiritual origin and as such requires spiritual intervention. In this part of Niger Delta of Nigeria there is a strong association between disease and witchcrafts, therefore she felt such disease should be treated by a witch doctor. We are hoping that within a short period she will present herself for definitive surgery. Reference
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm06014f1.jpg] |
| |||||||||
{kind=link}