 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
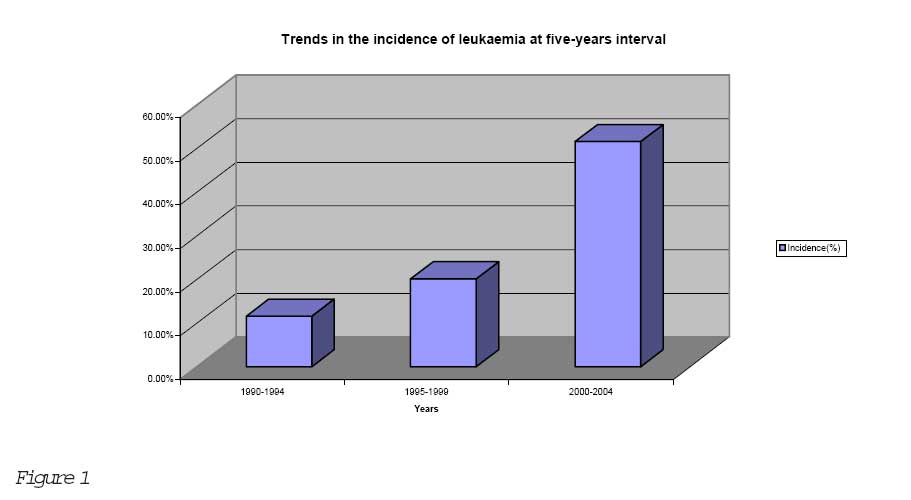
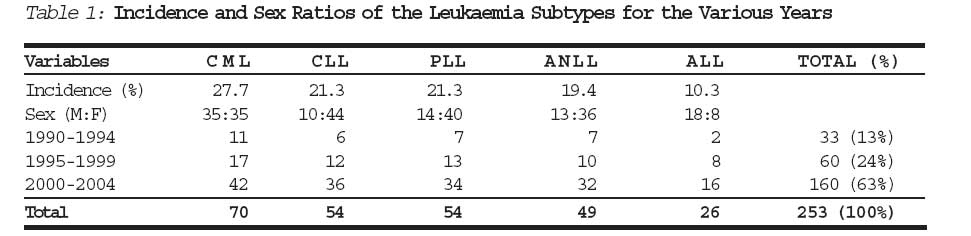
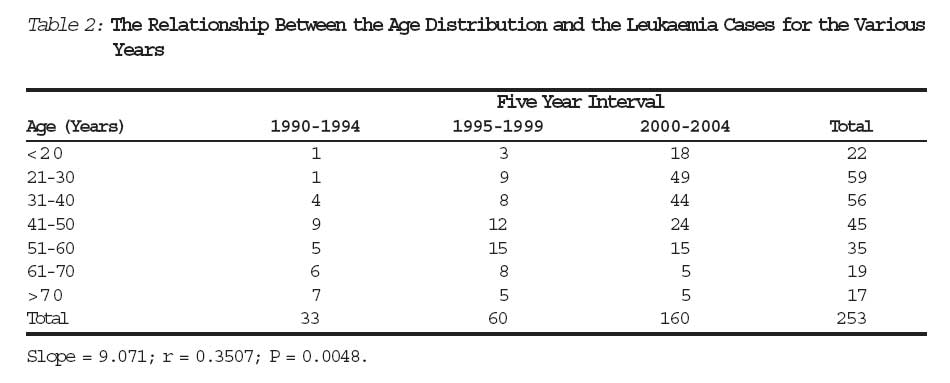
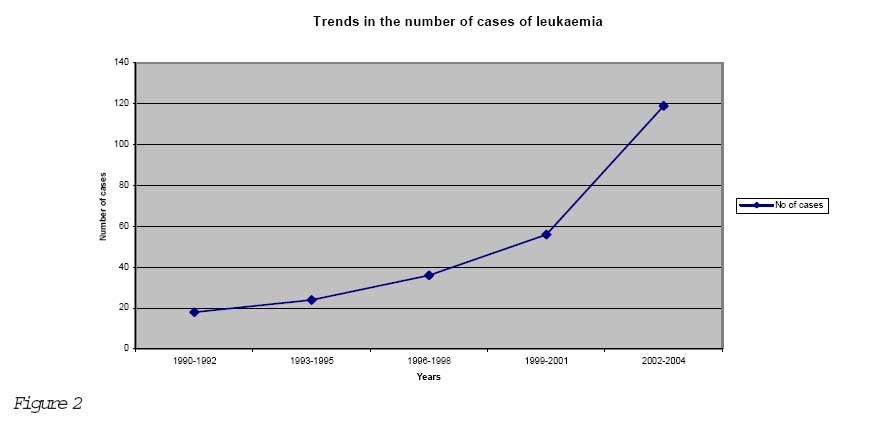
Journal of Medicine and Biomedical Research, Vol. 5, No. 2, December 2006, pp. 44-49 Trends in the Pattern of Leukaemia Incidence in a Tertiary Health Center in Nigeria: 1990-2004 aCaroline Edijana Omoti bEdwin Olatunji Imiere *Caroline Edijana Omoti and Edwin Olatunji Imiere MB.,BS., FMCPath Consultant Haematologist and Department of Haematology University of Benin Teaching Hospital, P.M.B. 1111, Benin City, Nigeria. E-mail: ediomoti @ yahoo.com Phone: 2348056014028. * Correspondence Code Number: jm06019 ABSTRACT Leukaemia is an important cause of morbidity and mortality in Nigeria. The aim of this study is to determine the incidence and trend in the pattern of adult leukaemia over a period of 15 years in Benin City, Nigeria. The case records of 253 cases that attended the University of Benin Teaching Hospital, Benin City, Nigeria from 1990-2004 with a diagnosis of leukaemia were analyzed. Chronic myeloid leukaemia (CML) was the more frequent variety (27.7%), followed by chronic lymphocytic leukaemia (CLL) and prolymphocytic leukaemia (PLL) with equal proportions of 21.3% each. Time trend analysis by 5-year calendar periods revealed an increasing number and incidence of patients with leukaemia. There was also an increased incidence of leukaemia among the youths (21-40years) whereas that of the older patients (61-70years) has decreased. There was a statistically significant association between age and number of leukaemia cases at presentation for the various years (P = 0.023). A positive correlation with a significant linear trend was also obtained (r = 0.3507; P = 0.0048) such that there was a predominance of young patients (21-40 years) in latter years (2000-2004) compared to a decline in the older patients (> 60 years) for the period studied. There was increased incidence of leukaemia especially among the younger age groups. Keywords: Leukaemia; trend; pattern; incidence. INTRODUCTION Leukaemias are diffuse clonal neoplastic disorders of the bone marrow and blood cells. They can be classified by immunologic, cytogenetic and molecular genetic methods into myeloid or lymphoid based on their origin and into acute and chronic depending on their clinical course.1 These methods can identify biologic subtypes requiring treatment approaches that differ in their use of specific drugs or drug combinations and duration of treatment required to achieve optimal results. The chronic leukaemias arise from the lymphocytic (chronic lymphocytic leukaemia, CLL) or myeloid (chronic myelogenous leukaemia, CML) precursor cells with their various subtypes. The acute leukaemias of multipotential primitive/progenitor cells are divided mainly into acute lymphocytic leukaemia, ALL and acute myelogenous leukaemia, AML/ANLL, acute nonlym-phocytic leukaemia. Chronic leukaemias (71.1%) has been reported to be more common than acute leukaemias (28.9%) in a study in Nigeria and other parts of Africa.2,3 They are not uncommon neoplastic disease in Nigeria (and indeed in Africa) and there is no doubt that adult leukaemia in Africa occurs as often as it does in the Caucasian.4,5 In a preliminary report of a prospective study of 113 haemo-poietic malignant patients seen at the University College Hospital, Ibadan, Nigeria, a proportion of 23.9%, 19.5%, 27.4% and 27.4% was estimated for AML, ALL, CML and CLL respectively.6 The Incidence rates (IR) of 0.9x10-5 and 1.9x10-5 were estimated for acute leukaemia and all leukaemia subtypes respectively.6 However, the incidence of ALL is higher in those of European descent than in those of Asia and African descent.7 In another study in Nigeria, of 146 leukaemic patients evaluated, 30.1% had CML, 23.3% had ALL, 22.6% had AML and 21.2% had CLL.4 There is a decline in mortality and higher probability of survival in the Western world due to advanced novel therapy protocol, early presentation by patients with availability of diagnostic tools.8 However, the same cannot be said for developing countries where the survival rate is very poor due to a number of strong limiting factors. The biological and epidemiological features including the socioeconomic status, differences in geographic, racial/ethnic and trend patterns of leukaemia subtypes in Africa have been identified.9 This suggests that the leukaemia subtypes may have different aetiologic factors.9 An epidemiologic study of the total number of patients with leukaemia in Benin City, Niger Delta region of Nigeria was performed with special emphasis on time trends because of the increasing westernization and industria-lization. This study aims to identify the incidence and time trends of leukaemia patients in Benin City, Nigeria. Patients and Methods The case files of all haematologic admissions were extracted from the medical records of the University of Benin Teaching Hospital (UBTH), Benin City, Nigeria, from 1990 to 2004 and those with a diagnosis of adult leukaemia were identified and the trend patterns were analyzed. The UBTH is a major referral center serving Edo and Delta states and other neighboring areas of the South-South geo-political zone of Nigeria. The pretherapy, clinical and demographic features were extracted from the case notes and analyzed including occupational history. The total number of haematological cases for each year was specially noted while the total number of all patients with leukaemia in the same time intervals was calculated. Diagnosis was established based on clinical information and cytological features of well-stained peripheral blood and bone marrow films using the Romanowsky (leishman) staining methods according to Dacie and Lewis.10 Other laboratory tests performed for the purpose of a leukaemia workup include complete blood counts, coombs test, immunologic studies which determine monoclonality, bone marrow and lymph node biopsy, serum protein electro-phoresis, blood cultures, electrolytes and urea, ultrasonography and cytogenetic study especially for patients in chronic phase CGL referred to OAUTHC, Ile-Ife in South Western part of the country for the possibility of Glivec (STI 571) therapy. The criteria for the diagnosis of prolymphocytic leukaemia (PLL) was according to Melo et al.11 The clinical presentation for CLL was staged according to the modified Rai12 and Binet13 clinical staging systems while the subtypes for acute leukaemias [ALL and AML] was based on the morphological criteria of the French-American-British (FAB) Cooperative group.14 Results The total number of haematologic admissions between 1990 and 2004 was 892 comprising at 5-year intervals of 284(1990-1994), 298(1995-1999) and 310(2000-2004). Out of these, the total number of leukaemia patients admitted was 253 comprising 33(11.6%), 60(20.1%) and 160(51.6%) respectively (Figure 1) which reveals the progressive time increase in leukaemia trends over the five-year interval periods. The catchment's population of the hospital is a total population of about 6.1 million. Analysis of the various subtypes of leukaemia showed that CML was the more frequent variety (27.7%), followed by CLL and PLL with equal proportions of 21.3% each. The incidence of ANLL was 19.4% while that of ALL was 10.3% (Table 1). A female prepon-derance (M:F) of 1:4.4, 1:2.9 and 1:2.8 was found for CLL, PLL and ANLL respectively while a male preponderance (M:F) of 2.3:1 was found for ALL. The 253 patients were aged 18-72years and mean age of 41.2 years (SEM±16.1) with peak age incidence at 21-40years (Table 2). This comprised of 90 males and 163 females with a male-to-female ratio of 1:1.8. The relationship between the age and the total number of cases for the 5-year intervals from 1990-1994 to 2000-2004 at diagnosis including the test for the linear trend is shown in Table 2. The mean overall number of cases for the 5-year interval was 4.71±1.13; 8.57±1.53 and 22.9± 6.65 with a median of 5.0, 8.0 and 18.0 respectively. There was a statistically significant association between age and the number of leukaemia cases at presentation for the various years (P=0.023) using the Kruskal Wallis nonparametric ANOVA test. A positive correlation with a significant linear trend was also obtained (r = 0.3507; P = 0.0048). The relationship was such that there was a predominance of young patients (21-40 years) in the latter years (2000-2004) while a large proportion of older patients (41-60 years) were seen in the earlier years (1990-1994). Figure 2 shows the progressive time trends in incidence of leukaemia at three-year intervals. Discussion The Environmental Impact Assessment data for the communities in the Niger Delta region of Nigeria that is known for its petrochemical industries and gas flare sites is of importance. This is because among all specific environ-mental pollutants, the chemical compounds released in petroleum industry hold the biggest interest with ionizing radiation and other leukaemogenic factors identified as aetiologic factors. Hence, the health status of the people is of great medical and socio-economic significance since they live close to the oil fields and gas flare sites. The chronic leukaemias (70.3%) were more common than the acute leukaemias (29.7%) with CML being the most common (27.7%) with a mean age of 38.8 years and equal number of patients in both sexes. This is similar to the finding in the same institution 5,15 and also in Ibadan, a large urban center in Southwestern rain forest area of Nigeria.4 In the Western countries however, CML accounts for 20% of the leukaemia subtypes while CLL accounts for 25% of cases.16 That leukaemia occurs more frequently in males has been reported17 but in this report it was more frequent in females with a female-to-male ratio (F:M) of 4.4:1, 2.9:1 and 2.8:1 for CLL, PLL and ANLL respectively. This female predominance (M:F=1:6) was also found in CLL patients in another part of the country.4 Only ALL with the least incidence of 10.3% had a male preponderance, which is known to have poor prognosis. The higher incidence of leukaemia in females could be because of improved enlightment and education allowing more females to present to hospitals. It has however been shown that females outnumber males in our hospital. This disparity has been attributed to a higher incidence of psychosomatism and a higher tendency to seek medical attention amongst females.18 It may also be because there are more females than males in Nigeria as shown by the census figures. Initially, leukaemia incidence rates were said to be higher in Caucasian than in the Blacks but recent reports revealed that the leukaemia is not an uncommon disease as it has been reported that adult leukaemia in Africa occurs as often as it does in the Caucasian.4 The total number of cases seen over the 15 year period from 1990-2004 shows a pattern of an increasing number and incidence for the various leukaemia subtypes. This increasing trend of leukaemia over the years can be described as due to a number of factors: improved awareness coupled with medical facilities for diagnosis, referral process including trained haematologists and treatment protocol which has improved over the years. Even when some seek alternative (traditional) therapy, they still eventually end up at late stages in the hospital, which is quite common. With increase in the population of Nigeria as the most populous Black Country in the world, there is also increase industria-lization with the production of toxic waste products and pollution of the air, water and land by industrial wastes dumpage of radioactive waste products on the coastal areas/shores. These complex patterns of change are different from those seen in some other advanced countries. In USA, the trend has shown an overall decline in incidence with recent reports suggesting an increasing trend for certain age and racial groups.19 This time trends highlight the likely importance of environmental factors in the aetiology of leukaemia. However, decline in mortality and higher probability of survival in the Western world has been linked to advanced novel therapy protocol, early presentation with wider use of tools for early diagnosis when it is most treatable. The number of cases seen with the young age group (21-40years) increased as the years progressed from 1990 to 2004 when compared to the older age groups. The difference in the age incidence observed in Nigerians when compared to the Western countries may be due to the interplay of both environmental (urbanization and industrialization) and racial factors.20 It could also be due to the pyramidal age structure of Nigeria with >50% of people less than 15 years. The younger age groups are the ones who have probably been exposed to petrochemical and other industrial waste since birth. The total mean number of cases increased from 4.71±1.13 for 1990-1994 to 22.9±6.65 for 2000-2004. A statistically significant increase in the number of cases of young patients in the latter years (2000-2004) was obtained (P = 0.023). There was also a correlation between the linear trend of age and the number of cases (r = 0.350; P = 0.0048) showing the preponderance of young patients in the latter years coupled with the increasing trend. This is similar to the study in USA where there was a proportional increase in the number of leukaemia in the youth.19 This observation is quite alarming and calls for renewed intensification of preventive measures/strategies as this is the working class group of a country. It spells doom for any nation as the productive and economically viable working class population is worst hit, thus destabilizing the manpower of the society. In conclusion, there is an increasing time trend in leukaemia among young age groups in contrast to a decrease in the older age groups during the period studied. This is probably due to exposure to petrochemical waste since birth, improved diagnostic efforts/ techniques, greater awareness and earlier presentation. Future research into the genetic makeup for female predominance in an African setting is advocated. Acknowledgement We wish to acknowledge the assistance of the consultants and residents in the Departmentof Haematolgy, University of Benin Teaching Hospital, Nigeria in the management of these patients. References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm06019t1.jpg] [jm06019f2.jpg] [jm06019f1.jpg] [jm06019t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}