 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
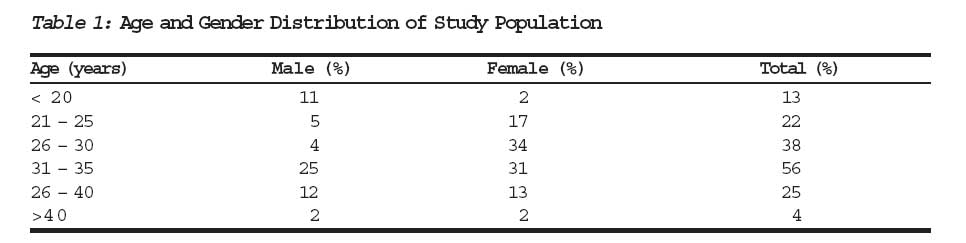
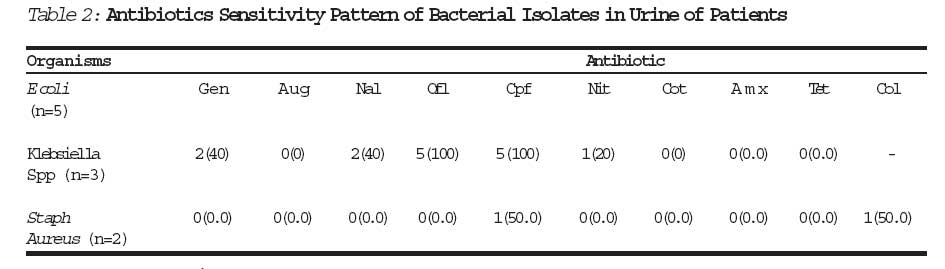
Journal of Medicine and Biomedical Research, Vol. 5, No. 2, December 2006, pp. 55-60 Urinary Tract Infection in Adolescent/Young Adult Nigerians with Acquired Human Immuno Deficiency Disease in Benin City Ibadin Okoeguale Michael Fmc Peada Onunu Abel FWACPb Ukoh G. M.scc aIbadin Okoeguale Michael Fmc Pead* Associate Professor of Paediatrics University of Benin Teaching Hospital Benin City Code Number: jm06021 Abstract In comparison with unaffected persons, individuals infected with HIV have undue predisposition to other infections including those of urinary tract. To assess this predilection to urinary tract infection (UTI) among this cohort, 158{59 (37%) males and 99 (63%) female} of them comprising mainly adolescents and young adults with confirmed HIV infection and attending Consultant Out patient Clinic of the University of Benin Teaching Hospital (UBTH) were evaluated for UTI through culture done on mid stream urine. The study carried out between September 2003 and May 2005 was prospective and cross sectional. Ten {(6.3%), one male and 9 females} patients had positive urine culture of uro-pathogenic organisms. Only 2 (20%) of these 10 patients had urinary symptoms of dysuria and loin pain. However fever was commoner among the patients with UTI as compared to those without it (54/148 or 36.5% vs 9/10 or 90.0%, χ2 =9.01, p<0.5). Urinary pathogens were Escherichia coli 5 (50%), Klebsiella species 3 (30%) and Staphylococcus aureus 1 (10%). In vitro sensitivity revealed that Escherichia coli and Klebsiella species were 100% sensitives to ofloxacin, 100% and 66.7% respectively to ciprofloxacin but completely resistant to cotrimoxazole, amoxicillin and clavulanic-acid potentiated amoxicillin. The adolescent/ young adult with HIV infection has enhanced risk of having UTI caused by similarly implicated organism in otherwise apparently health cohorts of comparable age bracket. Keywords: Urinary Tract Infection, Adolescents, Human Immunodeficiency Virus Introduction HIV/AIDS now ranks as one of the leading causes of morbidity and mortality in both children and adults.1,2 Since its advent in 1978 it has defiled every attempt at finding a permanent cure to it. Increasingly more persons are either infected or dying from it. Its ravaging stance however, is now almost confined to Africa and Asia.1,3 Human Immunodeficiency Virus is remarkable for its preference for T-lyphocytes and macrophages, which are rendered incompetent or depleted while opportunities are provided for organisms and agents of otherwise low virulence to establish them selves and cause various infections and further morbidities.4 Virtually every system in the body is susceptible in the course of evolution of the disease. Notable among these are skin, central nervous system, lungs and kidney. HIV nephropathy has been extensively documented both in adults and children.5,6 However there is paucity of literature on the role of the virus in predisposition to infections of the urinary tract.7 By its nature, the HIV predisposes to multi system/organ infection. It can thus be hypothesized that the incidence of UTI in individuals with HIV/AIDS would be increased in comparison to non-infected cohort. In this paper the prevalence of UTI in individuals with HIV/AIDS was assessed. Also evaluated were the implicated organisms and their in-vitro response to antibiotics. Patients and Methods The study which spanned a period of nine months (September 2003 _ May 2004), was carried out at the Consultant Outpatient Clinics of the University of Benin Teaching Hospital (UBTH), Benin City, operational only during week days. Study subjects were adolescents and young adults seen and managed on an outpatient bases for HIV/AIDS (stages 1&11). Patients were those managed in an adult ARV clinic by one of the authors (A.O). Young children under 12 years of age were not included. Also excluded were adults over 50 years of age because of increase chance of prostatism (in males) and increased incidence of UTI in older females. Some features of prostatism are also seen in UTL. Those who met the inclusion criteria but had access to antibiotics two weeks prior to enrolment in the study were excluded. Same applied to those with severe disease (stages 111 or IV commonly requiring in-patients care). Patients after due counseling designed to obtain verbal consent were enrolled consecutively over the period of study. From each patient the following were obtained. Bio-data, history of use of antibiotics, history of features suggestive of UTI, that is, dysuria, frequency, abdominal pain, flank pain and fever. Physical examinations carried out were also aimed and eliciting features that could implicate UTI (ie pyrexia and renal angle tenderness). Clean catch specimen of urine following due preparation of the urethra orifices in females or mid stream urine (MSU) in males was collected into a sterile universal container (with boric acid) from each patient. Such samples were transported almost immediately to the pharmaceutical Micro-biology labora-tory, Faculty of Pharmacy, University of Benin and worked upon within 4 hours of collection. Urine for culture including handling, staining and microscopy were carried out using standard procedures. In-vitro sensitivity testing (in situations where growth of single uro-pathogenic organism was found) was determined by the disc diffusion method.8 From the left-over urine specimen, urinalysis was carried out using Combi 10 (Macherey-Nagel) which examines for among others, protein, glucose, PH, erythrocyturia and ketones. Patients with positive culture were managed initially with clavulanic acid-potentiated amoxicillin but eventually treated according to the dictate of antibiotic sensitivity test where it was warranted. Data Analysis Tables of frequencies were drawn and proportions calculated for relevant variables. Mean and standard deviations were calculated for parametric variables. Incidences calculated in the study population were compared with values obtained from health population with comparable bio-data to allow inferences to be made using chi square test. P- Value less than 0.05 were considered significant. Results: The study carried out between September 2003 and May 2004 involved 158 adolescents and young adults with largely asymptomatic HIV infection being evaluated at the Consultant Outpatient Department of UBTH, Benin City. The study subjects were made up of 59(37%) males and 99(63%) females giving a male to female ratio of 2:3. the mean age was 30.3 ± 7.2 years, (range 15_45 years.) The modal age bracket was 25_30 years (Table I). Presenting Complaints The commonest complaints that could be ascribed to presence of urinary tract infection were urinary frequency 17 (10.8%). Others were loin pain 14 (8.9%), dysuria 12 (7.6%) and urgency 11 (7.0%). Though 63 (39.9%) had fever at point of evaluation, it was difficult to ascribe such solely to presence of UTI as fever could be indicative of primary disease or presence of secondary infection. None-theless 9/10 or 90.0% of those with positive cultures as against 54/148 or 36.5% of those with negative urine culture had fever. (cy2 = 9.01;p<0.05). Of the 10 persons who had positive urinary cultures, only 2 (20.0%) had urinary symp-toms of dysuria and loin pain. The remaining 8 (80.0%) were largely asymptomatic. Urinalyses Findings at urinalyses in these patients included proteinuria 45(28.5%), predomi-nantly white cell casts 23(14.6%), and significant pyuria (pus cells in excess of 4/ml)9(5.7%). Urinary pH was 5 in 82(51.9%) cases, 6 in 40(25.3%) cases but 7 and 8 in 19(12.0%) and 8(5.1%) cases respectively. The mean urinary pH of those without positive cultures 5.8± 0.8 did not vary significantly from the urinary Ph of those without positive cultures (5.6 ± 0.8). Besides the white cell cast which was significantly more in culture positive patients (5/10 or 50.0% vs 18/148 or 12.2%, χ2 = 9.8; p<0.05), other urinary findings were not significantly associated with presence of positive urine culture results. Nine (5.7%) of the 158 subjects had significant pyuria (5 or more pus cell per ml of centrifuged urine). Significantly more patients with UTI had significant pyuria as three or 30% of the 10 patients with positive urine culture as against 6/148 or 4.1% had significant pyuria. Urinary Culture and Sensitivity Pattern Ten patients had positive growth of uro-pathogenic organisms. This gave an incidence of UTI of 10/158 or 6.3%. Nine "(90.0%) of 10 cases with positive cultures were females. The urinary pathogens were Escherichia coli 5(50%); Klebsiella species, 3 (30.0%) and staphylococcus aureus, 2 (20%). Nine (90.0%) of those with positive cultures were females while only one (10.0%) was a male: The youngest of those with UTI was 22 years. (mean 29.0 ± 5.1years and range 22 _ 32 years). In vitro sensitivity pattern showed that Escherichia coli and Klesbsiella species were 100% sensitive to ofloxacin, 100% and 66.7% respectively sensitive to ciprofloxacin but completely resistant to cotrimoxazole, amoxicillin and clavulanic-acid potentiated amoxicillin. Response of Staphylococcus aureus to the quinolones and other commonly used antibiotics is as shown in Table II. Discussion An incidence of UTI of 6.3% as found in this study among adolescent / young adult cohort is significantly high in comparison with an average prevalence of 0.04% reported in otherwise healthy population of comparable ages.9 The increased incidence of UTI among patients with HIV is at tandem with the findings in the work of Schonwald.7 However, our finding of 6.3% is far lower than the 20.0% reported in the study carried out by Kaplan et al.10 The latter study was conducted among AIDS (symptomatic HIV) patient in comparison with predominantly asympto-matic HIV cases perhaps suggesting an association between degree of immune suppressions and prevalence of UTI. To corroborate this assertion of increased incidence in more profoundly immuno-compromised individuals are the findings of the work of De Pinho et al11 where 13.3% of frankly AIDS patients in contrast to 3.2% in patients with asymptomatic HIV infection had UTI. The increased incidence of UTI among such patients could be explained on the basis of general immuno-suppression which is the hallmark of HIV/AIDS.12,13 The immuno-suppression predisposes to infection in various body systems. The involvement of the kidney in such widespread morbidity pattern would therefore not be a surprise. Our finding however is at variance with what Asharam et al14 found among children with HIV. The authors had noted that there was no significant impact of HIV/AIDS on the presentation or incidence of UTI in children _ an observation that one can not readily explain as a more profound suppression of immunity would have been expected in children with concomitant increase in incidence of UTI. Perhaps the fact that the older patient is more liable to live longer grants him higher chances of developing renal complications. The preponderance of females among patients with UTI as found in this study is in agreement with most studies on UTI particularly outside infancy. The pheno-menon is explained by many factors including short urethra and close proximity between the anal orifice and the urethra opening in females in comparison with males. Other Urologic Manifestations About twenty eight per cent of our patients had proteinuria but only 0.03% of these were significant proteinuria in contrast to the 22.0% prevalence of significant proteinuria reported by Kaplan et al.10 Kaplan et al10 also noted a 52.0% prevalence of pyuria in contradis-tinction to the 5.6% noted in our series. Again it is uncertain why the wide variation in the prevalence of proteinuria and pyuria between these studies. Of note however is the finding that thirty per cent of pacients with pyuria had UTI. Pyuria as an indication of inflammatory process and occurring significantly more among patients with UTI is at tandem with most reports on UTI.15,16 It may serve as screening tool in situations where culture is not immediately feasible. Presence of urinary casts occurred more significantly in patients with UTI than those without it. Previous works did not comment on the relationship between incidence of UTI and presence of urinary cast in patients with HIV/AIDS. However the increased incidence of urinary casts among such patients may be indicative of the widespread involvement of renal tissues including tubules in the disease process. It may also represent side effects of some of the anti retro viral drugs some of the patients would have had access to.13 Uropathogens The urinary isolates of Escherichia coli, Klebsiella species and Staphylococcus aureus in the study varied markedly from those noted in similar studies that included Salmonella spp10, Acinetobacter calcoaticus10, Enterococci, Pseudomonas aeruginosa17 and Mycoplasma spp.18 Most organisms reported in these series are fastidious, requiring specialized media for growth. Such facilities are lacking in our center. It is therefore uncertain if such organisms also contribute to the prevalence of UTI among this cobort in our study location. Bacterial isolates in this study are similar to those commonly implicated in UTI in our study location, perhaps suggesting that HIV/AIDS patients suffer increased morbidities from common organisms as well as being perhaps predisposed to infections caused by rare bacteria. The prominence of Escherichia coli as noted in this study is in conformity with the findings contained in the works of De pinho10 among men with AIDS. Of particular importance is the in-vitro sensitive pattern of the strains of bacteria isolated. Widespread resistance of isolates to common antibiotics were demonstrated while only ofloxacin and perfloxacin showed appreciable coverage against same organisms _ a trend that had been noted by Manfredi et al.17 The trend may also be a reflection of the changes in antibiotic sensitivity pattern recently noted in UTI in association with other morbidities in same study locale that has been ascribed to widespread self medication and indiscriminate use of antibiotics15 _ practices that are likely to be more with patients having HIV/AIDS. In conclusion HIV/AIDS predisposes the adolescent/young adult to increased incidence of UTI caused by same organisms that are commonly implicated in otherwise healthy cohort of comparable age bracket. However the uropathogens performed poorly in in-vitro sensitivity to commonly used antibiotics. Acknowledgement We wish to thank the doctors in the paediatric renal unit and those in the Consultant Out patient Clinics for their contributions through sample collection. The immense contributions of the staffers of the Department of Pharma-ceutical Microbiology, Faculty of Pharmacy through handling of samples are appreciated. References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm06021t2.jpg] [jm06021t1.jpg] |
| |||||||||
{kind=link}
{kind=link}