 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
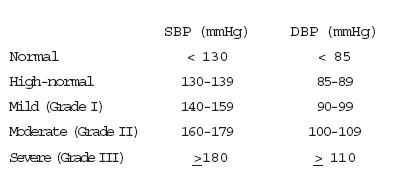
Journal of Medicine and Biomedical Research, Vol. 5, No. 2, December 2006, pp. 79-86 Blood pressure pattern and prevalence of hypertension in a rural community in Edo State aOmuemu VO, aOkojie OH and bOmuemu CE Departments of Community Healtha and Medicineb, College of Medicine, University of Benin, P.M.B. 1154, Benin-city, Edo state Nigeria. Correspondence to: Dr. V. O. Omuemu e-mail: cvomuemu@yahoo.com Code Number: jm06025 ABSTRACT This cross-sectional study was carried out in Udo, a rural community in Ovia South-west LGA of Edo state to screen for hypertension and determine blood pressure pattern. Cluster sampling method was used in selecting participants. Data collection was by researcher-administered questionnaire. Blood pressure and anthropometric measurements were determined. A total of 590 respondents with mean age 30.7 ± 14.6 years participated in the study. Mean systolic and diastolic blood pressures were 122.08 ± 15.42 mmHg and 79.54 ± 11.55 mmHg, respectively and increased with age. Males had significantly higher mean SBP and DBP than the females (p < 0.001). Prevalence of hypertension was 20.2%, increased significantly with age and was higher in males than in females (p < 0.001). This study revealed that hypertension is a problem even in the rural areas. Therefore need for intervention programmes targeted at non-communicable diseases like hypertension which is usually symptomless. Keywords: Blood Presure, Pattern, Hypertension Introduction Hypertension is one of the chronic non-communicable diseases that is being recognized as an emerging public health problem in the developing countries including Nigeria.1 Defining hypertension can be arbitrary because there is no clear dividing line between normal blood pressure and raised blood pressure in the general popu-lation nor between levels of blood pressure which are harmful and those which are not.2 In adults, it is generally agreed that a blood pressure is abnormal when the systolic pressure is equal to or greater than 140 mmHg and diastolic pressure is equal to or greater than 90 mmHg.3 It is not just a disease in itself but also a risk factor for the development of several cardiovascular, cerebrovascular and renal diseases.4,5 The impact of hypertension on the lives of people is enormous when measured in terms of morbidity, mortality and economic loss to the individual, family and nation as a whole. It significantly impairs life expectancy; the higher the blood pressure, the greater the reduction in longevity. In the Framingham cohort, the risk of developing coronary heart diseases rose progressively with increasing systolic pressure or diastolic pressure both in middle aged and the elderly.6 The prevalence of hypertension depends on the racial composition of the population studied and the criteria used to define the condition. Also, in any given population, the proportion of people who are aware of their high blood pressure status is usually low7-10 since the condition is often without symptoms. It is in view of this that this study was carried out to screen for hypertension and determine blood pressure pattern in Udo (a rural community in Ovia south-west LGA of Edo state) with the hope that those who are hypertensive will benefit by seeking early management. Materials and methods This cross-sectional and descriptive study was carried out in Udo which is a rural community. It is one of the 126 communities in Ovia South-west LGA of Edo State. Udo is about 40 km from Benin-city, the state capital and about 8 km from Iguobazuwa, the local government headquarter. The people are Binis and speak the Edo language. There is a traditional ruling system with the headship being referred to as 'Iyasere'. The people are mainly engaged in agricultural activities especially crop farming. The study population included all males and females aged 15 years and above who are resident in the community. The minimum sample size was calculated using the formula for calculating sample size for a descriptive, cross-sectional study N = pq/(E/1.96)2 where p = prevalence of hypertension = 11.2%7 and q = 1 - p. The minimum sample size was 153, however, a total of 590 respondents participated in the study. A cluster sampling method was carried out using a quarter as a sampling unit. Two out of the nine quarters were selected by simple random sampling (balloting) and all males and females aged 15 years and above in the selected quarters were included in the study. Pretested, interviewer-administered ques-tionnaire was the tool for data collection. Interviewers had a common training programme conducted by the principal investigators. The training included standardization of methods of questionnaire administration, measurement of blood pressure and anthropometric indices. This was to ensure accuracy, reduce inter- and intra-observer errors and ensure comparability of blood pressure and study participants' responses. The sphygmomanometers, weighing scales and meter rule used were all standardized. Blood pressure measurement: The blood pressure was measured using Accoson mercury sphygmomanometer and for accuracy the following steps were adopted:2 The individual was rested for at least 5 minutes in a sitting position with the arm rested on a table such that the middle of the right arm was about the level of the heart and any tight clothing removed from the arm. The cuff was inflated, palpating the radial artery and the inflation was continued until 20-30 mmHg above the disappearance of the radial pulse. The stethoscope diaphragm was placed over the brachial artery in the ante-cubital fossa and the cuff deflated, allowing the mercury to fall gradually, about 2 mmHg per second. The first sound (Korotkoff 1) was taken as the systolic blood pressure and the extinction of all sounds (Korotkoff 5) as the diastolic blood pressure. The blood pressure was recorded to the nearest 2 mmHg. Two blood pressure readings were taken at an interval of 15 minutes and the mean of the two readings taken as the individual's blood pressure measurement. The blood pressure pattern in the study population was classified using the WHO/ISH defined criteria for blood pressure and hypertension:3
Height measurement: The height was measured with a measuring tape, the subject standing erect without shoes and the back against a wall. Head coverings were removed. This was recorded in meters to two decimal points. Parallax effect in height measurement was avoided by fitting the measuring tape with a sliding head-piece at right angles to the upright, which was lowered onto the subject's head.11 Weight measurement: The body weight was measured with a simple bathroom scale with light clothes and without shoes. This was recorded in kilogrammes to one decimal point. Scale adjustment error in weight measurement was avoided by adjusting the pointer to zero (with a knob in the weighing scale) before placing and weighing each subject. The zero was checked each day and the calibration assessed by reference to an individual of known weight. Also the scale was placed on a firm horizontal surface. Smokers included those who smoked regularly and at least one cigarette on the average during the previous 30 days while non-smokers were lifetime abstainers and occasional smokers. Alcohol drinkers included individuals who took any amount of alcohol while non-drinkers included only abstainers. Physical activity was assessed using open-ended questions inquiring about average activity during work and leisure time and was classified into 3 groups:12 Not active physically: desk top jobs, petty trading Moderately active physically: house-hold chores, hawking, tailoring, walking to school or place of work. Very active physically: farming/field work, jogging, cycling to school or place of work. Data analysis was by computer using the SPSS statistical package and differences were considered significant at p less than 0.05. Multiple logistic regression analysis was performed to study the correlates of hypertension. Hypertension status was the dependent variable. Age, sex, marital status, educational status, body mass index (BMI), smoking, alcohol drinking were the independent variable. Stepwise selection was used for model building and the significant T value 0.100 was selected criteria for removal at each step of the regression. Results The demographic profile of the respondents is shown in Table 1. A total of 590 respondents were involved in the study in Udo community, comprising of 355 (60.2%) males and 235 (39.8%) females. The mean age of the respondents was 30.7 ± 14.6 years. The mean systolic blood pressure (SBP) for the total population was 122.08 ± 15.42 mmHg and this increased with age. The diastolic blood pressure (DBP) for the total population was 79.54 ± 11.55 mmHg and this also increased with age. Mean SBP for the male respondents was 124.54 ± 14.81 mmHg and was signifi-cantly higher than that for the females, 118.37 ± 15.61 mmHg (t = 4.78, p < 0.001). The mean DBP was significantly higher for the male respondents (81.50 + 10.67 mmHg) than for the female respondents (76.58 ± 12.20 mmHg), t = 5.07, p < 0.001. It was also noted that below the age of 45 years, the mean SBP was higher in males than in the females and as from 45 years onwards, the females had a higher mean SBP. (Table 2) The same was also observed for the mean DBP. (Table 3). Table 4 shows the blood pressure pattern of the study population classified according to the WHO/ISH criteria. Overall, 63.7% of the study population had normal blood pressure with the males having a lower proportion of such individuals than the females. A total of 16.9% of the study population had high-normal blood pressure with the higher proportion being noted in the males. Overall, 13.4% of the study population had mild hypertension (Grade I) (16.6% of males and 8.5% of females), 3.7% of the study population had moderate hypertension (Grade II) (5.6% of males and 0.9% of females), 2.2% of them had severe hypertension (Grade III) (1.7% of males and 3.0% of females). The prevalence of hypertension in this study population was 20.2% using the WHO/ISH criteria of SBP equal to or greater than 140 mmHg and/or DBP equal to or greater than 90 mmHg. This was significantly higher in males (24.8%) than in females (13.2%), X2 = 11.81, p < 0.001. The prevalence of hyper-tension increased with age from 8.4% in those 15-24 years of age to 63% in those 65 years and above and the difference was statistically significant (X2 = 75.79, p < 0.001). This was observed for both males and females. It was also noted that below 55 years of age, the prevalence of hypertension was higher in the males than in the females while as from the age of 55 years, the female respondents had a higher prevalence. (Table 5) The results of the multiple regression analysis done showed that body mass index (BMI), marital status, age and educational status were all correlates of hypertension. After controlling for age, a higher BMI was significantly associated with hypertension (Adjusted O.R = 1.91 (95% CI = 1.71 to 3.13), X2 = 7.079, p = 0.008. Being ever married and in the lower educational status were weakly associated with a high blood pressure [Adjusted O.R equals 0.63 (95% CI = 0.32 to 1.24), X2 = 1.689, p = 0.194] and 1.13 (95% CI = 0.70 to 1.82), X2 = 0.225, p = 0.635], respectively. (Table 6) Gender, cigarette smoking, alcohol consumption and physical inactivity were not predictors of high blood pressure. Discussion All the respondents were aged 15 years and above with a mean age of 30.7 ± 14.6 years. This is close to the national average as demonstrated in the 1991 national census (31.6 ± 14.1 years).7 The population was predominantly male as they constituted 60.2% of the total population. The results from our study showed that the mean systolic blood pressure (SBP) and mean diastolic blood pressure (DBP) increased with age. This is in agreement with previous reports from several studies.13-16 Overall, the mean SBP and mean DBP were higher in the male respondents than in the female respondents. The differences were statistically significant (t = 4.78, p < 0.001 and t= 5.07, p < 0.001, respectively). This trend has been reported by other studies.16-18 Blood pressures of different age groups in both sexes were compared. Below the age of 45 years, the mean SBP and mean DBP were higher in the males than in the females. Above this age, the mean SBP and mean DBP were higher in the females than in the males. This has been shown in other studies.16,17,19 This trend is known to be due in part to the hormonal changes which occur at menopause. The prevalence of hypertension in the study population was 20.2%. This is higher than the prevalence of 8-10% reported by Akinkugbe in rural communities in Africa20 and the prevalence of 5.9% reported by Oviasu in a rural community in mid-western Nigeria17 and 11% reported by Kuti in Aiyetoro community (also rural) in Ondo state.19 It is also higher than the prevalence of 9.8% reported in the national survey on non-communicable diseases in 1992.7 The much higher prevalence recorded in our study population could be due to the fact that the cut off for hypertension in our study was 140/90 mmHg compared with 160/95 mmHg7,19,20 and 160/100 mmHg17 that were used in the previous studies. This now highlights the increasing burden of hyper-tension in the nation which must be tackled urgently and seriously. This is even more so that about 16.9% of the study population had a high-normal blood pressure. It was also observed that the prevalence of hypertension increased with age which is in agreement with reports from several studies.7,13-15,18 This was expected since blood pressure tends to increase with advancing age due to hardening of the arteries. This trend of increasing blood pressure with age could also be a reflection of increasing risk factors for hypertension such as obesity which also increases with age.21,22 Overall, the prevalence of hypertension was significantly higher in the male respondents (24.8%) than in the female respondents (13.2%), X2 = 11.81, p < 0.001). This is comparable to findings in other studies.16,17,23 This pattern was seen before the age of 55 years, thereafter, the prevalence was higher in the females respondents than in the males. This is a reflection of the blood pressure pattern among males and females in the study community. This may be attributed in part to hormonal changes in the females as they approach menopause or may be due to decreased survival in older hypertensive men. The association of hypertension with a high body mass index,7,18 and a lower educational status24,25 in this study population has been documented. This study has once again highlighted the fact that hypertension is a problem in our society, even in the rural areas. A lot of attention is focused on the control of commu-nicable diseases while the non-communicable ones like hypertension go unchecked. There is need for programmes targeted at control of non-communicable diseases like hyper-tension, which is symptomless. Members of rural communities should have access to Information Education and Communication (IEC) on hypertension to facilitate regular screening to detect and initiate treatment earlier as well as promotion of a healthy lifestyle that may prevent or delay its onset and complications. Acknowledgement The authors would like to thank the members of Udo community for their co-operation during data collection. Our sincere gratitude is also extended to Drs Iyamu and Aghedo for their assistance. References
© CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm06025t4.jpg] [jm06025t1.jpg] [jm06025t3.jpg] [jm06025t2.jpg] [jm06025t6.jpg] [jm06025t5.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}