 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
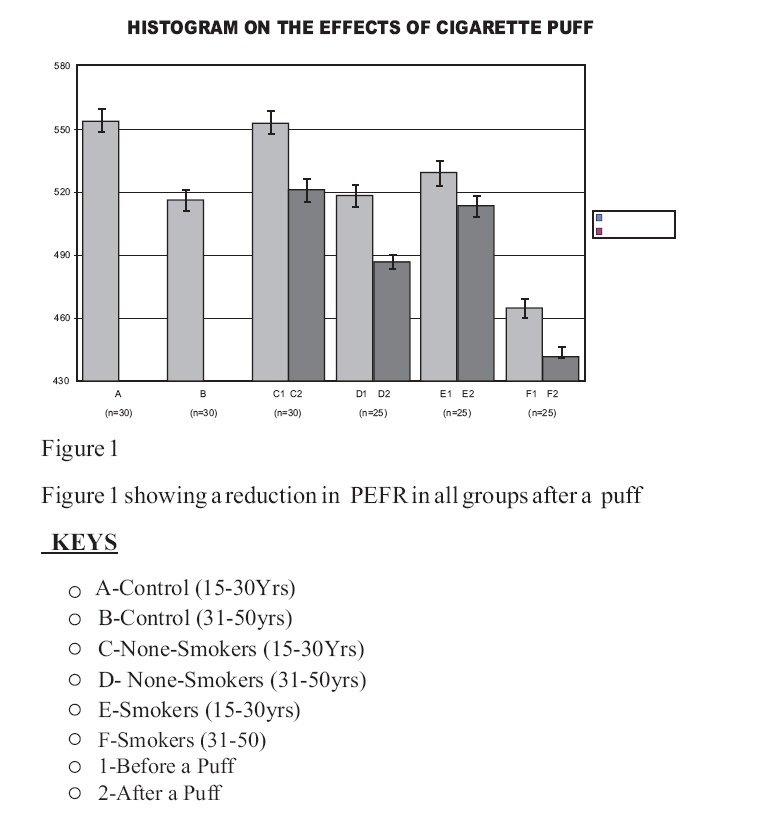
Journal of Medicine and Biomedical Research, Vol. 6, No. 1 & 2, December 2007, pp. 4-12 The Effect of a Single Cigarette Puff on Air Flow in the Lungs. VI Iyawe , CN Ejindu , MI Ebomoyi and HA Oboh2 Departments of Physiology and Medical Biochemistry,
School of Basic Medical Sciences, College of Medical
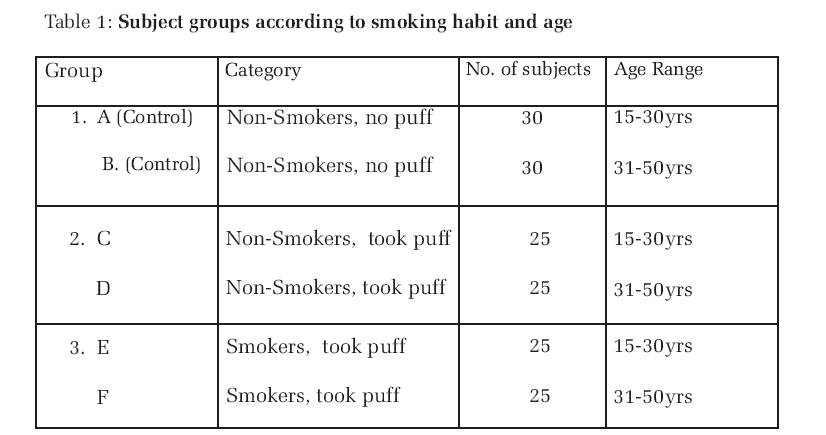
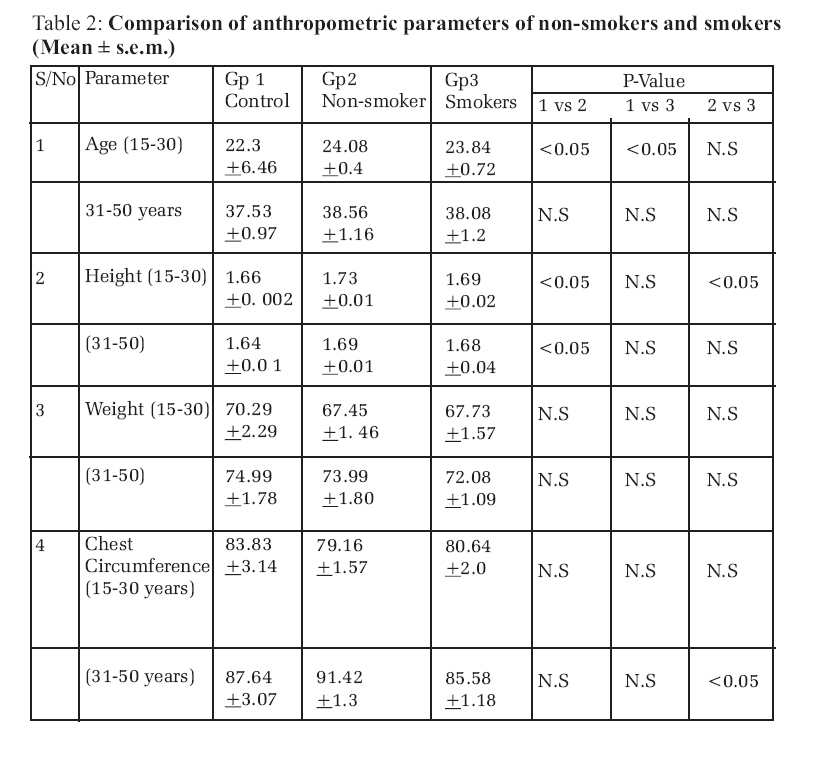
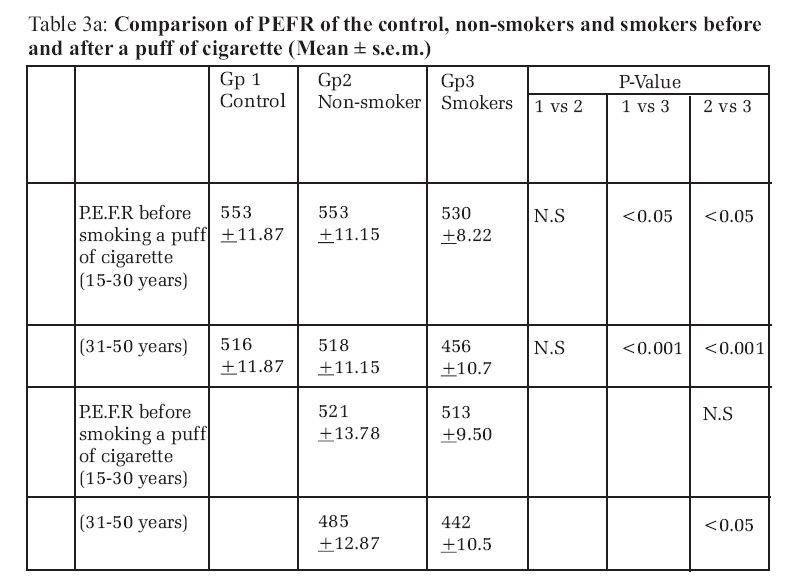
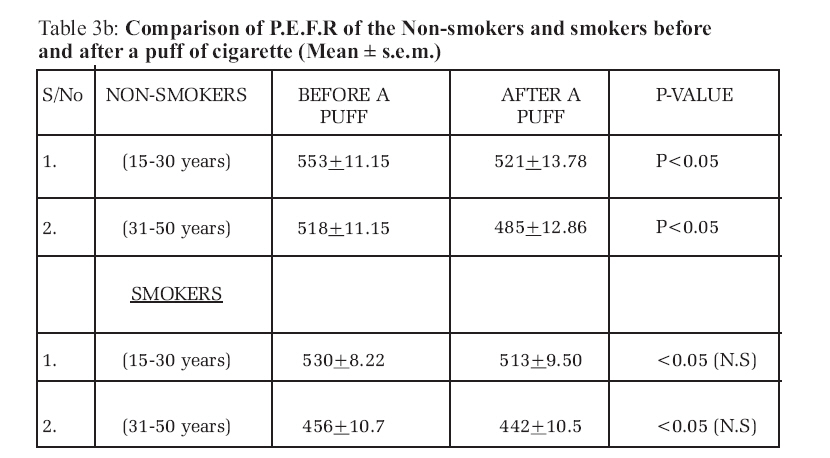
Sciences, University of Benin, Benin City, Nigeria. Code Number: jm07001 ABSTRACT Peak expiratory flow rate (PEFR) was measured in 160 apparently healthy males, 15 50 years of age, consisting of 60 non-smokers (control) and 100 who volunteered to smoke (experimental subjects). Out of the 100 subjects, 50 who were also non-smokers smoked a cigarette through a single suck (puff). Another 50 who previously smoked also took a single puff. Results indicate that PEFR for the control group was 558 ± 10L/min in the 30 younger subjects (15-30yrs) and 516 ± 11 L/min in the 30 older subjects (31 50 years) and the difference was significant (P<0.05) The initial PEFR for smokers before they took a puff was significantly lower than for non-smokers (P<0.05). After a puff, there was no significant difference in PEFR between the smokers and non-smokers in the younger group. In the older group, PEFR of smokers was lower than those of non-smokers (P<0.05). Overall, a puff of cigarette significantly reduced PEFR in non-smokers, but the reduction in PEFR following a single puff in smokers was not significant. KEYWORDS: PEFR, Cigarette puff. INTRODUCTION Cigarette is produced from tobacco. The tobacco plant is believed to have originated in the western Hemisphere1 . The plant is grown for its leaves, which can be smoked, chewed or sniffed for a variety of effects. It is considered an addictive substance especially because of its nicotine content. When a cigarette is lit, it emits smoke which contains nicotine and over 19 known carcinogens (most, collectively known as “tars”) and more than 4,000 chemicals2 . A puff of cigarette is estimated to contain 1016 oxidants. The degree of smoking or smoke exposure can be ascertained by measuring the serum levels of continine (a metabolite of nicotine) Despite knowing that inhaling cigarette can seriously damage the health of humans, its social importance has grown over the years, even to the point of denoting the “modern or liberated woman” in the western world during the twentieth century1 . Cigarette smoking is a major component of indoor and outdoor air pollution causing environmental tobacco smoke and secondary smoking in other people. It contributes to a remarkable number of diseases, including coronary heart disease, stroke, chronic obstructive airway disease, peptic ulcer, peripheral vascular disease and many types of cancers3 . Thus smoking affects several systems of the body, most especially the first line organ, the lungs. The harmful substances which enter the lungs, spread through the body and can reach the brain, heart and other organs within 10seconds of the first puff.2 Inhalation of cigarette puff has an immediate effect on respiration by increasing airway resistance and therefore reducing the amount of oxygen absorbed into the body.4 Smoking causes a chronic (or long term) swelling of mucous membranes, which also leads to increased airway resistance. It induces chronic irritation of the respiratory lining and wide variety of carcinogens in the cells lining the respiratory tract. These changes lead to cancer. 5 Smoking greatly affects the lungs from an annoying repeated cough to grave illnesses like chronic bronchitis, emphysema and bronchial carcinoma.6 The risk to the respiratory system, especially the risk of cancer continues to plague the ex-smoker for years after quitting. There is increased incidence of asthma in children of smoking mothers.7 There is also retardation of the rate of lung development and lung function in these children and those involved in childhood and adolescent smoking.4 The above effects on the respiratory system are well known in chronic smokers. The acute effect of cigarette smoke is not well documented. The present study, therefore, examines the effect of cigarette smoke (a single suck or puff) on air flow in the lungs, by measuring PEFR soon after the puff. PEFR is generally considered as a sensitive indicator of changes in elastic recoil pressure and/or inflammatory change in the bronchiolar walls.8 MATERIALS AND METHODS The work was carried out in Benin City using staff and students of the University of Benin. A total of 160 subjects, all males volunteered for the study. Females refused to participate in the study. This was not surprising since smoking by females is not an acceptable social habit in Nigeria. Also, it was difficult to get more male volunteers because of the scare of the 'diseases' associated with cigarette smoking, However, the volunteers were divided into groups according to their smoking habits and ages. The 160 males consisted of 60 nonsmokers who served as control (Gp1 A and B), 50 non-smokers who took a puff (Gp2 C and D) and 50 smokers who took a puff, (Gp3 E and F). Each of the 3 groups was subdivided into two equal groups based on ages 15-30 years and 31-50 years (table 1). Prior to any measurement, questionnaires eliciting information on age, medical history and smoking habit was administered. The height, weight and chest circumference were recorded. As in many health surveys, only one parameter was measured, the PEFR, that is, the fastest rate of exhalation which gives an indication of airway resistance. A Wright Peak Flow meter was used in the measurement. Volunteers gave informed consent for the study and Ethical Committee approval was obtained. Subjects were made to practice and perfect the required breathing manoeuvre before recorded measurements of PEFR were taken. The test was carried out in all the subjects in the sitting position. The highest PEFR from three attempts was recorded and used for analysis.9 PEFR was measured in the subjects before and after a puff of cigarette except in the controls in whom PEFR was measured without inhalation of cigarette smoke. The subjects were trained in the act of 'puffing'. Each puff of cigarette lasted for approximately 2 seconds and measurements of PEFR started 10 to 15 seconds after the puff. For the smokers, a smoke free interval of 24 hours was observed before the puff and PEFR measurements. The data were subjected to statistical analysis and P values calculated using the students t-test. RESULTS The results are presented as mean and standard error of mean (tables 2 and 3a and b). Overall, the age, height, weight, and chest circumference of non smokers and smokers were not significantly different (table 2). PEFR of the younger subjects was higher than those of older subjects. There was no significant difference between the PEFR of non-smokers and control in the two age groups (1 vs 2, table 3a). However, there was a significant reduction in the PEFR of nonsmokers of both groups after taking a puff (p < 0.05) (table 3b) and figure 1 (Gps C and D). For smokers, their initial PEFR were lower than those of the control (table 3a, 1 vs 3 and 2 vs 3). The lower values in comparison with control were more pronounced for smokers in the older age group (P < 0.01). Furthermore, a comparison between smokers and non smokers shows that the PEFR of smokers was lower than those of non smokers (P < 0.05) for both age groups (table 3a and b). When the smokers took a puff, there was a reduction in their PEFR, like those of the non smokers, but the reduction was not significant (figure 1, Gps E and F). DISCUSSION The present study was designed to examine the effect of cigarette puff on lung function. It is unique in that it focuses on the acute response to a single puff of cigarette smoker. It has the advantage that the volunteers do not inhale a large quantity of smoke which can be deleterious to their health. The measured index, PEFR, is generally considered as a sensitive indicator for changes in elastic recoil pressure and/or the resistance to airflow in medium and small airways.10,11 It has been known that various indices of lung function including FEVI and PEFR decrease over time in smokers. 12,13 Furthermore, inhalation of cigarette smoke has an immediate effect on respiration by increasing airway resistance.14 Exposure to environmental tobacco smoke (E.T.S.) or passive smoking leads to reduced lung function,6,15 increased risk of lower respiratory tract illness and acute exacerbation of asthma.16 The findings of this study for the normal control group are in conformity with those of previous studies on Nigeria.17,18,19 However, the PEFR of the three groups (control, non-smokers and smokers) were significantly higher in the younger age group than the older ones. This is attributable to the effect of age on lung tissues. With age, the expiratory muscles used for it hard to exclude latent diseases in the older age group.20 Also, the PEFR is subject to wide variabilities. These include height, weight, and chest circumference. In this study, these variables did not make significant contribution to the effect of the puff. Height and chest circumference might have affected the PEFR, but the marked changes in PEFR cannot be attributed to these variables. The study reveals a significant reduction in the PEFR of non-smokers after taking a puff of cigarette. On the other hand, the decrease in PEFR of smokers after a puff was not significant. Smokers have a lower level of lung function than those who have not smoked.21 The smokers had a low basal PEFR. Hence no significant reduction after a puff. How does cigarette smoke increase airway resistance and decrease PEFR? Several mechanisms exist. First, it can be attributed to rapidly responding receptors within the airway causing bronchoconstriction and tachypnoea. Secondly, the accumulated effect of tobacco smoke is an increased load of oxidants in the respiratory tract, both directly by inhalation of oxidants in the smoke and indirectly by activation of inflammatory cells.22 Thirdly, smoking significantly increased progressive deterioration of the lung functions and is a risk factor in chronic obstructive pulmonary diseases, in which pulmonary mechanics deteriorates and causes loss of elastic recoil of the lungs and slowing forced expiration. 4 Fourthly, with nicotine, mucus-producing cells grow in size and number, so that the amount of mucus secreted is more and also thicker.4 Fifthly, cigarette smoke slows the movement of cilia on the airway epithelium and also reduces their number, making mucociliary clearance difficult and further clogging up the airway.23 Furthermore, nicotine promotes tumor growth and angiogenesis in adults. It can induce angiogenesis by activating nicotinic acetylcholine receptors (nAchRs) on the surface of endothelial cells which stimulates their proliferation and the subsequent formation of blood vessels.24 Cigarette smoke also increases levels of chemo attractant protein and vascular endothelial growth factor which also aid angiogenesis and tumour growth.25 It is now known that cigarette smoke can induce remodelling in the trachea in the absence of inflammation. Some form of airway remodeling might have been established in the older smokers.26 CONCLUSION In conclusion, PEFR was reduced after a puff of cigarette. Smoking status influenced the PEFR value as smokers had substantially lower values at the outset of the study. It is well known that from a puff of cigarette, smokers move to a stick and then from sticks to addiction and so the effects accumulate. The effect of tobacco smoking can be deleterious. If a single puff increases airway resistance and reduces PEFR, chronic smoking is bound to do much damage to the lungs. References
© Copyright 2007 - CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm07001t3a.jpg] [jm07001t2.jpg] [jm07001t1.jpg] [jm07001t3b.jpg] [jm07001f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}