 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Medicine and Biomedical Research, Vol. 7, No. 1 & 2, December 2008, pp. 5-11 A Study of Personality And Psychological Distress Among Delusional Halitosis Patients. a Akhigbe K. O.; aKoleoso O. N.; bAkpata O.; bOmoregie F.O a Department of Mental Health, University of Benin Teaching
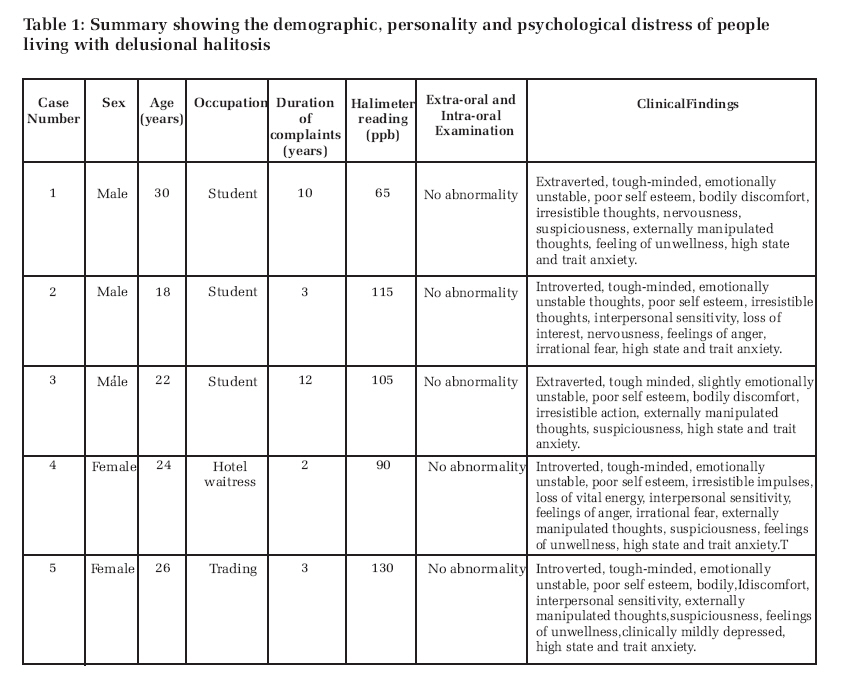
Hospital. Benin City. Code Number: jm08001 ABSTRACT An assessment of personality and psychological distress of people living with delusional halitosis attending Oral Wellness Centre (OWC) at the University of Benin Teaching Hospital, Benin City over a six-month period was undertaken. Five (5) patients with age range of 18-30 years and a mean age of 24 years (SD = 4.47) were included in the study. These individuals manifested multiple symptoms associated with distress and they experienced personal discomfort and social embarrassment leading to emotional distress. The study highlights the importance of assessing personality characteristics and psychological dysfunction of patients presenting with delusional halitosis. A multidisciplinary approach in the treatment of delusional halitosis cannot, therefore be overemphasized. KEYWORDS: Oral malodour, Personality characteristics, Pychological distress, Delusional halitosis, Volatile sulphur compounds. INTRODUCTION Halitosis is a general term used to describe an unpleasant or offensive odour emanating from the oral cavity. Although, the non-oral sites related to oral malodour include the upper and lower respiratory tracts, the gastrointestinal tract, and some diseases involving the kidneys or the liver; about 90% of all bad breath emanate from the mouth itself1, 2 . Bad breath may have an oral or extraoral etiology, but it usually originates in the patient's mouth. The strong disagreeable odour arises from volatile sulfur compound, mainly hydrogen sulfide (H2S) and mercaptans, produced by the decomposition of proteins (amino acids containing the - SH group) under the influence of anaerobic, gram-negative bacteria. Remains of food, shed and inflammatory cells, blood and postnasal drip consist of proteins. The decomposition of these proteins generally takes place in areas where the presence of proteins and anaerobic bacteria is made possible by the normal anatomy (e.g. furrowed mucosa covering the dorsum of the tongue, interdental spaces, valleculae, piriform recesses) or by pathological changes (e.g. gum pockets). The dorsum of the tongue is the principal source of volatile sulfur compounds in the oral cavity. Extraoral causes of bad breath include diseases of the lungs, esophagus and nose, systemic diseases affecting the liver and kidneys, and diabetes. A considerable proportion of patients presenting with a complaint of chronic bad breath suffer from imaginary halitosis. 3 When dealing with patients seeking professional care for halitosis, one must be prepared to differentiate between these patients. There are those patients who emit above average malodour, those who emit average or near average malodour but are more sensitive to it, and those who emit below average or no odour but believe that their breath is offensive despite objective evidence to the contrary. Whereas the former two cases warrant treatment for malodour, in the latter, it is not necessary. 4 Many patients who complain of chronic bad breath have no objective evidence of breath malodour. 5 Olfactory Reference Syndrome is a psychiatric condition in which there occurs a somatization of some distress resulting in a belief on the part of the patient that an offensive odour emanates from some body part usually the mouth. This condition described in the psychiatric literature for over 100 years, interferes with normal social interactions because of fear of offending others with breath malodour. 6,7 Several studies8-10 reported that Affective Disorders and Schizophrenia develop in patients whose initial complaints were limited to breath malodour, and some success has been reported in treating olfactory reference syndrome with tricyclic antidepressants and the neuroleptic pimozide. Real or imagined possession of bad breath might lead to a limitation of social contacts, particularly since it is very difficult to smell one's own breath and testing it by breathing into the hand held in front of the mouth and nose is generally ineffective. In those who suffer from imaginary or delusional halitosis, it is the inability to be sure whether or not halitosis is present that makes them very unhappy.11 Breath malodour is a condition that has health and social implication rendering it an area of oral science that spans medical and psychological issues. Current social norms emphasize the importance of personal image and interpersonal relationships. In this context, breath malodour may be an important factor in social communication and therefore, may be the origin of concern not only for a possible health condition but also for frequent psychological alterations leading to social and personal isolation. 12 Patients affected by delusional halitosis never wish to visit a psychologist or psychiatrist, because they cannot recognize their own psychosomatic condition. They also never doubt that they have offensive oral malodour. These patients interpret other people's behavior, such as covering the nose or averting the face, as an indication that their breath is offensive, and these behaviours or attitudes reinforce their belief that they have a strong oral malodour. 13 The population in the western countries is becoming more concerned and paying more attention to the problem of bad breath, due to the importance of social interactions in contemporary society. This has reflected in the result of a telephone survey carried out in the United States, where 60% of American women and 50% of American men referred to using cosmetic breath freshening products. 14 However, in spite of this general concern and the possible psychosocial implication of delusional halitosis, health professionals, including dental professionals, psychiatrist and clinical psychologists are poorly informed about this condition. Therefore, they are unable to treat or properly advice people with delusional halitosis. The aim of this study is to present the personality characteristics and the psychological distress of people suffering from delusional halitosis. In addition, the study aims to correlate the findings with the reported psychosocial problems associated with this condition. This could afford clinicians a better understanding of these people, so that appropriate therapeutic intervention can be determined. It may also give emphasis to the joint role of the general dentist and the mental health professionals as the most appropriate professionals to diagnose and manage this condition. PATIENTS AND METHOD Design This article employs the case study design based upon experiences reported in details, so that the description captures as much of the unique characteristics of the individual and his or her situations. Participants/Setting This study involved patients referred to the Oral Wellness Centre (OWC) at the University of Benin Teaching Hospital, Benin City over a six-month period (April to September 2004). The OWC is a multidisciplinary outpatient team offering oral malodour assessment, consulting and treatment. The centre receives referrals from other dental departments within the hospital. The patients before referral to OWC have had extensive treatments for bad breath in other medical and dental clinics. Thus, they have typically been complaining of halitosis for months, if not years, prior to referral. As part of the clinical assessment of these patients in this centre, detail history, clinical examination and breath measurement using halimeter (RH-17 Series by Interscan, USA) were performed. The patients were also required to complete a packet of self -report questionnaires consisting of instruments used for mental health assessment. Instruments The instruments used for collecting data for the study are as follows:
Eysenck Personality Questionnaire (fourth version).15 E P Q consists of 90 items, designed to measure four aspects of personality namely, Psychoticism, Extroversion, Neuroticism and Lie scale. Symptom Distress Checklist 90.16 This is a 90-item inventory designed to assess 10 primary categories of symptoms associated with distress among psychiatric outpatients and with the experience of anguish arising from the problems of living among people in the general population. These ten categories of symptoms are somatisation, obsessive compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism and neuroticism. Spielberger's State-Tract Anxiety Inventory, or STAI. 17 This consists of 40 statements, 20 of which measure trait anxiety and 20 state anxiety. Self-Rating depression Scale. 18 This is a 20-item self-reporting scale designed to assess the cognitive, affective, psychomotor, somatic and social interpersonal dimension of depression. It categorized depression into mild, moderate, severe and profound depression. Index of Self Esteem. 19 This is a 25item inventory, designed to measure the self-perceived and self-evaluative component of self-concept, which is the sum total of the self-perceived and the other-perceived views of the self held by a person. The Halimeter reading. The Halimeter is an instrument that measures the volatile sulphur compounds emitted from the mouth. These sulphur compounds are the products of the anaerobic bacterial degradation of sulphur containing amino acids within the oral cavity, and include hydrogen sulphide (H2 S), methyl mercaptan (CH3SH),and dimethyl sulphide (CH 3 SCH 3 ), collectively referred to as volatile sulphur compounds (VSC). The Halimeter responds to all three volatile sulfur compounds, and gives a reading of total VSC's and the reading is in parts-per-billion (ppb) of volatile sulfur compounds. A reading of 80 to 140 ppb is considered as normal range. Readings lower than this range are still indicative of no oral malodor, and are otherwise clinically inconsequential. Procedure Each patient referred to the centre had a package of self-report questionnaires to fill. Thereafter, the dentists in the team examined them extra-orally and intra-orally and carried out a Halimeter assessment of their breath. The psychiatrist and clinical psychologist then carried out mental state examination and a comprehensive psychological assessment of the patients respectively. RESULTS We present five typical cases of delusional halitosis within the study period, consisting of three males and two females, with age range of 18-30 years and a mean age of 24 years (S.D.4.47). A summary of findings is given in Table 1. Case 1: A 30-year old male student who presented at the clinic with 10 years history of bad breath, associated with sipping saliva from upper single tooth denture. Patient claimed that people particularly the opposite sex turned away their faces when speaking with or to him and some even openly complained about his bad breath. Extra-oral and Intra-oral examination however showed no abnormality. Clinical examination of exhaled breath did not indicate oral malodour. Halimeter assessment of patient's mouth breath of 65 ppb was lower than the normal range. Psychological assessment of patient revealed an individual who was extraverted, tough-minded, emotionally unstable and had poor self-esteem. High score on the psychological distress scale suggested that patient manifested Somatization, obsessive compulsiveness, Anxiety, Paranoid ideation, Psychoticism and Neuroticism. The patient's state anxiety level is also high, though there was no manifestation of clinical depression. Case 2: An 18-year old male student who presented at the clinic with three (3) years history of bad breath with associated bitter taste on the tongue. Patient also claimed that people have been avoiding him and placing finger over their nose when having discussion with him. He had stopped attending school a few weeks before presentation. Extra-oral and Intra-oral examination showed no abnormality. Clinical examination of exhaled breath did not indicate oral malodour. Halimeter assessment of patient's mouth was within normal range (115 ppb). Personality assessment shows an individual that was tough-minded, introverted, emotionally unstable and had poor self-esteem. Symptom Distress Checklist indicated such psychological complaints as obsessive compulsiveness, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety and paranoid ideation. The patient's anxiety level as a general aspect of personality and as a response to a specific situation as measured by STAI was high. There was no clinical depression in the patient. Case 3: A 22 years old male student who presented with 12 years history of bad breath with associated dental deposits of his teeth, which was persistent even after repeated dental cleaning over the past three (3) years. Extra-oral and Intra-oral examination showed no abnormality. Clinical examination of exhaled breath did not indicate oral malodour. Halimeter assessment of patient mouth breath was 105ppb and this was within normal. Personality assessment score suggested a person who was tough-minded, extraverted, slightly emotionally unstable and poor self-esteem. His score on SCL-90 implied the presence of somatization, obsessive compulsiveness, psychoticism and paranoid ideation. The patient's general level of anxiety is high, likewise his predisposition to being anxious. There was no clinical depression. Case 4: A 24 years old female hotel-waitress who presented with 2 years history of bad breath following sexual intercourse with her boy friend. The condition made it difficult for her to interact freely with customers. Extra-oral and Intra-oral examination showed no abnormality. Clinical examination of exhaled breath did not indicate oral malodour. Halimeter reading of patient's mouth breath was within normal (90ppb). Her performance on EPQ suggested an individual who was tough-minded, introverted and emotionally unstable. She also had poor self-esteem. SCL-90 revealed high score on obsessive compulsiveness, depression, interpersonal sensitivity, hostility, phobic anxiety, psychoticism, neuroticism and paranoid ideation. High score on STAI reflected the presence of both state and trait anxiety. There was no evidence of clinical depression. Case 5: A 26 years old female trader who presented with 3 years history of bad breath associated with bitter taste. She claimed that people avoided her and turned their faces away when speaking with her. Extra-oral and Intra-oral examination showed no abnormality. Clinical examination of exhaled breath did not suggest oral malodour. Halimeter reading was normal (130 ppb). Assessment of her personality using EPQ showed she was tough-minded introverted and emotionally unstable. Index of Self Esteem Scale showed she had poor self-esteem. Her level of psychopathology as measured by SCL-90 revealed that she somatizes, with interpersonal sensitivity and was depressed. She also suffered from paranoid ideation. The patient's situation specific emotion and her predisposition to being anxious were high as indicated by STAI. Clinically, she was mildly depressed. DISCUSSION Overall analysis of the personality characteristics and psychological complaints of people suffering from delusional halitosis revealed gross multiple symptoms associated with distress and experience of anguish arising from the problem of living. The extra-oral and intra-oral clinical assessment and the halimeter investigations showed no breath abnormality in all the patients studied. Similarly, previous reports have identified persistent complaint of chronic bad breath without objective evidence of oral malodour as the diagnostic criteria for delusional halitosis. 3-5,11 All the patients presented in the study manifest the following distress: toughmindedness, emotionality, suspiciousness, poor self-esteem and high anxiety to a specific situation. Four out of the five patients showed evidence of irresistible thought impulses and action, and high predisposition to being anxious. Meanwhile, bodily discomfort, discomfort in social situation, loss of interest in usual activities and externally manipulated thought were present in three of the five patients. This agree with previous studies 4,11,12 of this condition that highlighted the possible effects of all forms of halitosis on social interaction and communication of affected individuals. In addition, extraversion, nervousness, feelings of anger, irrational fear and feelings of unwellness were present in two of the patients. However, only one delusional halitosis patient showed evidence of mild clinical depression. This suggests that these patients are very emotional and rarely suffer depression. This study is novel in its own right. It appears to be a pioneering study. As far as the authors are aware, there are no reports of similar studies from an African population. Nevertheless, some observations made in the course of the study were significant. This study has been able to prove that people living with delusional halitosis exist in our environment and these individuals experience personal discomfort and social embarrassment leading to emotional distress just like people with real chronic oral malodour.4,12 Dentists and mental health experts were involved in the management of all the patients studied. This further emphasized the need for a multidisciplinary approach in the management of delusional halitosis.20 It is important for dentists and mental health professionals to be aware of the personality characteristics and psychological complaints of these patients as part of their overall presentation, to ensure reliable diagnosis and appropriate treatment for this condition. In conclusion, the study highlights the importance of assessing personality characteristics and psychological dysfunction of patients presenting with delusional halitosis. Therefore, a multidisciplinary approach in the treatment of delusional halitosis cannot be overemphasized. This study is however limited due to its case study approach. References
© Copyright 2008 - CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm08001t1.jpg] |
| |||||||||
{kind=link}