 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
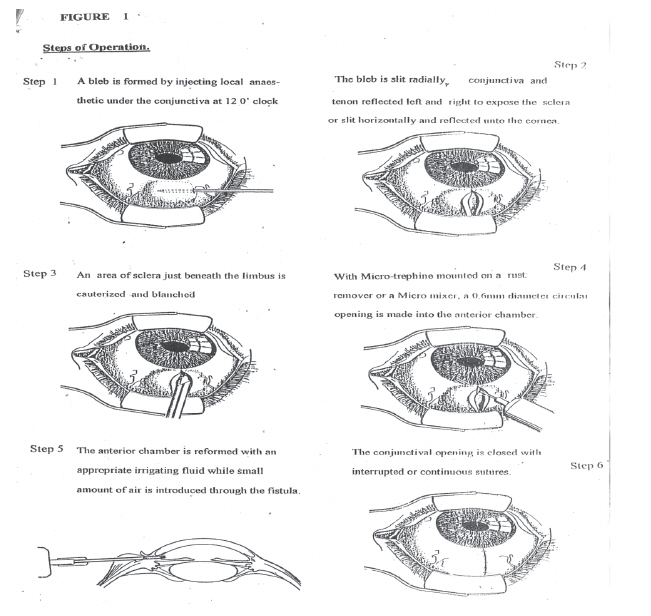
Journal of Medicine and Biomedical Research, Vol. 7, No. 1 & 2, December 2008, pp. 16-23 Micro-trephination Glaucoma Surgery In Nigerians: 10 Years Outcome *Dr. Joseph Momodu Waziri-Erameh , Dr. Afekhide Ernest Omoti Department Of Ophthalmology, University Of Benin Teaching Hospital, PMB 1111 Benin City Nigeria.Email: Repwaziri@yahoo.com. Code Number: jm08003 ABSTRACT The aim of this study was to show the effectiveness of microtrephination glaucoma surgery in Nigerians followed up for up to 10 years. Eight eyes of 5 Nigerian patients who had microtrephination glaucoma surgery at DDS Eye Surgery, Benin City and the University of Benin Teaching Hospital Benin City were followed up for at least 10 years. The visual acuity, cup disc ratio and intraocular pressures were monitored in each eye. Intraocular pressure was measured by applanation tonometry in all cases. Two eyes (25%) had adequate intraocular pressure control and did not require additional medications after 10 years. The remaining 6 eyes (75%) did not have satisfactory intraocular pressure control and needed additional antiglaucoma medication. Micro-trephination appears to be unsatisfactory for effective control of intra-ocular pressure in Nigerian eyes. However the great potential of microtrephination making glaucoma surgery affordable and available to Nigerians and other developing countries may still be realizable. What may be required is to determine the appropriate diameter of the trephine that strikes adequate balance between preventing hypotony and obliteration. KEYWORDS: Micro-trephination, Glaucoma, Surgery Intra-ocular pressure INTRODUCTION Glaucoma is now generally accepted as a group of optic neuropathies typically characterized by visual field loss and structural damage to the optic nerve fibre. High intra ocular pressure (IOP) previously one of the tripods of diagnosis is now regarded a major risk factor for glaucoma development but it remains the most clinically tangible aspect of the disease1 . The number of people with primary glaucoma in the world by the year 2000 is estimated at nearly 66.8million, with 6.7million suffering from bilateral blindness2 . In sub-Saharan West Africa including Nigeria, glaucoma is a devastating and often under diagnosed problem. It is a leading cause of blindness second only to cataract3 . Treatment of glaucoma is difficult and reducing IOP further is the main objective target of glaucoma management. Reduction of IOP methods comprise medication or surgery or combination of both. Surgical managements is currently being advocated for Africans as it has been shown that chronic anti glaucoma medication is detrimental in the long run to glaucoma treatment 3. Issues of availability, cost, genuiness and compliance make wide spread use of anti glaucoma medications impractical 2. A spectrum of surgical techniques for glaucoma treatment exist but many of them have gone into abeyance. Elliot in 1903 described full thickness trephination . 4The technique was very successful in lowering IOP, but the trephine diameter of 1.5mm was too large and it led to severe hypotony and other consequent complications. Cairnes in 1968 described trabeculectony7 as a partial thickness filtering glaucoma surgery and was modified by Watson in 1970 8. It is presently the most popular glaucoma surgery technique. It is said to have a success rate that is above 65% . 9 It is however a major ophthalmic surgery, complex, expensive, less affordable, less available and failure rates are especially high in blacks. Microtrephination glaucoma surgery (MTGS) was introduced in the late 1980s by Singh as a fistulizing procedure10. It is also a full thickness trephination only unlike that introduced by Elliot, the microtrephine has diameter of 0.6mm and addresses the problems of over drainage and severe hypotony associated with the 1.5mm diameter trephine. It also has the advantage of being cheap, simple, easy to use and the potential for large scale surgery in camp settings. The satisfactory early outcome of the first eleven Nigerian eyes that had MTGS was published in 2002 after a follow up period of 3 months to 36months11. This article is on the outcome of eight of those eyes 10 years after the MTGS at the University of Benin Teaching Hospital (UBTH) and DDS Eye Surgery Benin City. Materials, Methods and Patients The materials, methods and patients are essentially as described in the preliminary report of the first eleven Nigerian eyes that had microtrephination glaucoma surgery (MTGS) at DDS Eye Surgery and the UBTH Benin City 11(the steps of the operation are as shown in figure 1). The eyes were anaesthetized with a retrobulbar injection of 3mls of 2% lidnocaine (+ 1:120,000 adrenaline) or the conjunctiva infilterated with 1ml of lidnocaine + adrenaline at the chosen surgery site. The conjunctiva was reflected either fornix or limbal based and the area cauterized to the bare sclera. The 0.6mm diameter trephine mounted on a battery operated micro mixer drills a 0.6mm circular hole into the anterior chamber through the sclera. A peripherial iridectomy was performed through the trephine opening with a fine forceps and the conjunctiva closed over the opening with 8/0 or 9/0 sutures. The anterior chamber was reformed through the trephine opening or through a paracentesis opening. The eye was padded after antibiotic and steroid eye drops were instilled and the patient discharged home. On the first post operative (post-op) day, the eye pad wass removed , eye examined for vsual acuity (VA), anterior chamber depth and intra ocular pressure (IOP) amongst others and the patient discharged with the eye unpadded if all was well. All the patients were chronic open angle glaucoma (COAG) patients with these other inclusion criteria :-
For the 10 years post MTGS assessment, effort was made to locate the patients and in the case of a patient who lived very far away from Benin City, an Ophthalmologist colleague in the same town was provided the patient's contact address and assisted with the IOP measurements. All IOP measurements were with the applanation tonometer. Patients who had MTGS and were on antiglaucoma medication for effective control of their IOP had their medication discontinued for one week before the IOP measurement to eliminate as much as possible the effect of anti glaucoma medication on the IOP. The medication was resumed immediately after the IOP measurement. Other preoperative measurements included visual acuity (VA), cup disc ratio (CDR), intra Ocular pressure (IOP) of the right eye (RE) and left eye (LE) respectively. RESULTS This article is on eight Nigerian eyes followed up for 10 years after micro-trephination glaucoma surgery (MTGS). They were the first patients in Nigeria to undergo MTGS. The follow up period ranged from 10 years and 18 days to 10 years and 9 months. Three of the original eleven eyes were excluded from this study for they were lost to follow up before 10 years. Six of the 8 eyes (75%) had unsatisfactory average pressure reduction 10 years after the MTGS and are on anti glaucoma medications while 2 eyes had satisfactory pressure reduction 10 years after the MTGS and were not on anti glaucoma medications. The 8 eyes from 5 patients had their IOP measured 10 years after their MTGS. Some patients who kept their clinic appointments also had their IOP at 5 years recorded in this study. Patient A was a 39yrs old male. At time of surgery
Comment. This patient had successful MTGS. The eye is not on anti glaucoma medication and the patient keeps regular clinic appointments. The patient is an oil company worker who had trabeculectomy in the RE two years before the MTGS. He opted for MTGS for he did not want the long hospital stay he experienced with the trabeculectony of the RE because of hypotony. Patient B. was a 60yrs Female at time of surgery.
Comment: This patient had unsuccessful MTGS in both eyes. Patient was lost to follow up after 2 yrs but surfaced recently because of cataract in the LE that has resulted in light perception vision. Patient is on antiglaucoma medication and IOP are about 27mmHg in both eyes. Patient C was a 74yrs female. At time of surgery:
Comment: Ten years after MTGS pressure reduction is about 15mmHg. This was successful surgery. Patient D: was a 72 yrs male. At time of surgery:
Comment: Patients MTGS failed by the 12th month post op and has been on antiglaucoma medication. Patient E: was a 24yrs male. At time of surgery:
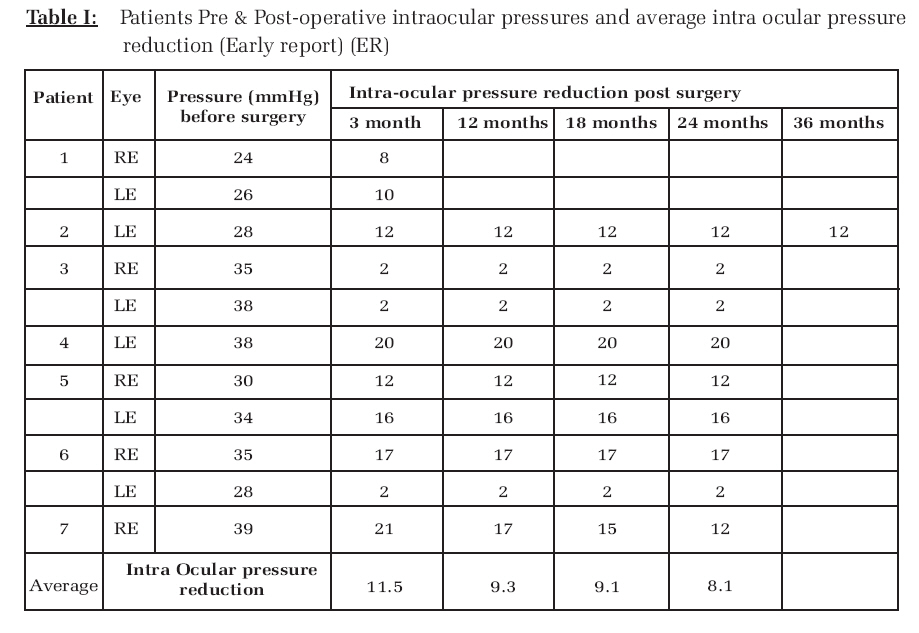
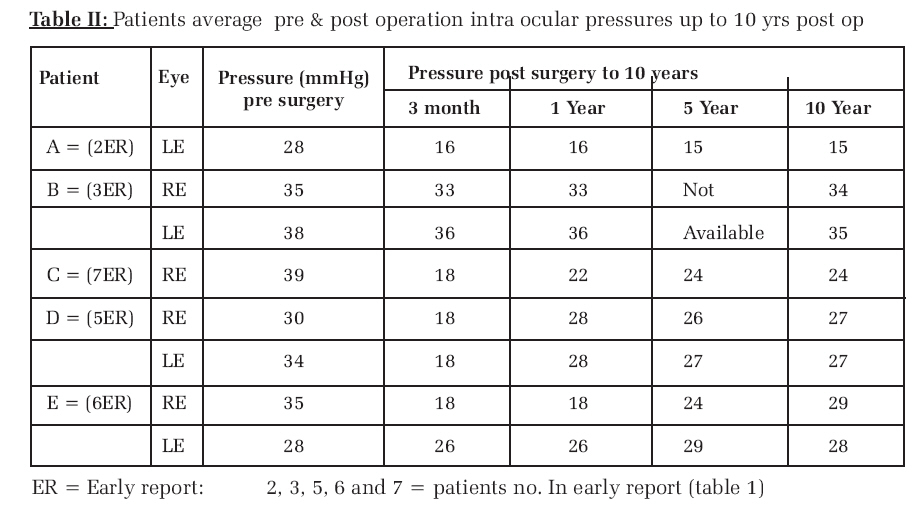
Comment: The right eye had double trephine holes at time of surgery. At 1 yr it had a reduction of 17mmHg, but at 10yrs the reduction has fallen from 17mmHg to 6mmHg showing a gradual failing of the MTGS. The double trephine holes may be responsible for the apparently fairly successful result. The LE had only one trephine hole. It failed by the first year. Patient is on antiglaucoma medication. The double trephine holes may be responsible for the relatively more successful outcome in the RE compared with the LE. DISCUSSION Micro trephination glaucoma surgery promises great potentials. The procedure is inexpensive and is easy to carry out with less than 1ml of local anaesthetic. Unlike the popular trabeculectomy which is a major ophthalmic surgery, the patient does not need to be admitted, and vision is back to normal in one to two days. MTGS could also be a surgery adjunct to medical treatment of glaucoma similar to laser trabeculoplasty in advanced economies with out the burden of cost and reduced effectivity in blacks after laser trebeculoplasty.12 The first eight Nigerian eyes from 5 patients who had MTGS and IOP assessed 10yrs after the surgery are the subject of this study. The report on the early experience with MTGS had an average follow up period of 2 years (table I) The early report was very promising. Five eyes had very satisfactory IOP reduction while 4 eyes had absolute success using the criteria of IOP not greater than 22mmHg and IOP reduction greater than 5mmHg.13 The early report also showed that the MTGS stabilized by 12 months as shown by average intra ocular pressure reduction of 9.3mmHg at 12 months, 9.1mmHg at 18 months and 8.8mmHg at 24 months. This study is on the outcome of MTGS 10years after. We found a not too encouraging pattern where only two patients of the 8 patients assessed for IOP after 10 years can be said to have good success with IOP less than 22mmHg and IOP reduction more than 5mmHg (table II). In the early report, the trend of waning effectivity with time was already obvious with an average reduction of 9.3mmHg at 12 months, 9.1mmHg at 18 months and 8.8mmHg by 24 months. The observed trend of failing of the procedure with time may not be unconnected with gradual obliteration of the 0.6mm trephine hole. This finding is explainable by the high fibroblast activities encountered in African and Asian eyes after trauma including surgery. 14,15,16 The high fibroblast activities in African eyes have been adduced for failure of filtering procedures in Africans.17 Patient E showed a gradual loss of effectivity of the procedure from a mean reduction in IOP of 17mmHg at 2 years, 11mmHg at 5 years and 6mmHg at 10 years post MTGS. This decline may have been slowed down as a result of the double (experimental) trephine hole carried out on this patient. The challenge is to carry out further studies to determine what diameter of trephine will strike a proper balance between being adequately wide enough to prevent hypotony and also wide enough to prevent early obliteration by fibroblast activities in African eyes. Another possibility is the intra-operation application of mitomycin C during MTGS to significantly suppress fibroblast activities. Sergienko and Torchinskaia18 have described having considerable success with application of mitomycin C intra operatively but this is yet to be followed for as long as 10 years. Singh10 working with Indian eyes had considerable long-term success. In conclusion, the great potential of MTGS making glaucoma surgery affordable and available to Nigerians and other developing countries though in doubt by the results of this study, is still realizable. What is required is the overcoming of fibroblast activities obliterating the 0.6mm trephine hole or determining the appropriate diameter that strikes adequate balance between preventing hypotony and obliteration of the trephine hole. References
© Copyright 2008 - CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm08003f1.jpg] [jm08003t1.jpg] [jm08003t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}