 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Medicine and Biomedical Research, Vol. 7, No. 1 & 2, December 2008, pp. 58-65 Prevalence of Malocclusion Among School Children in Benin City, Nigeria Emmanuel O. Ajayi a Orthodontic Unit, Department of Preventive Dentistry,
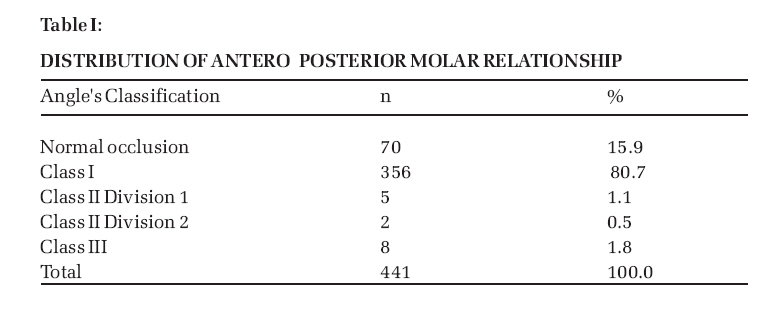
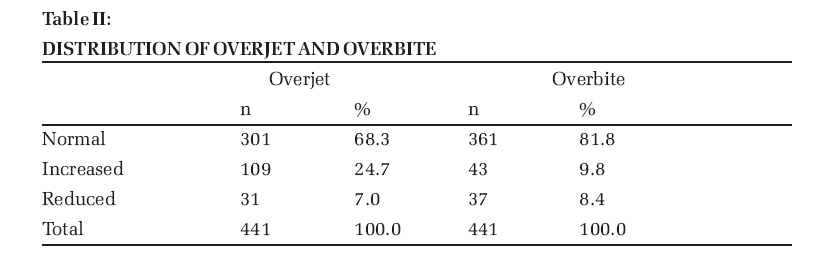
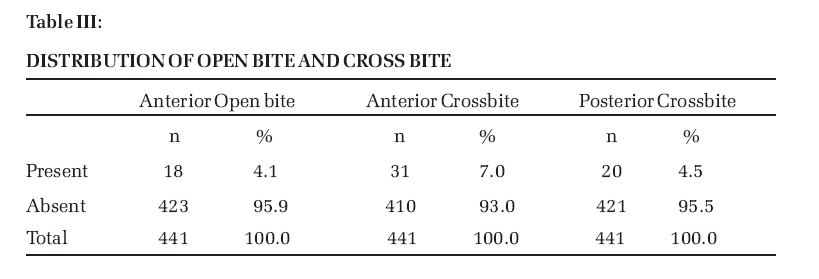
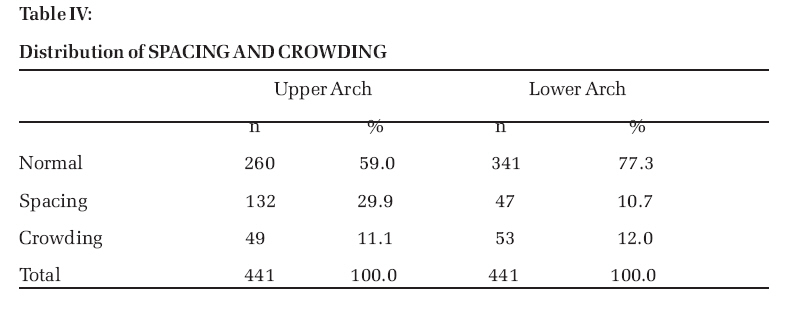
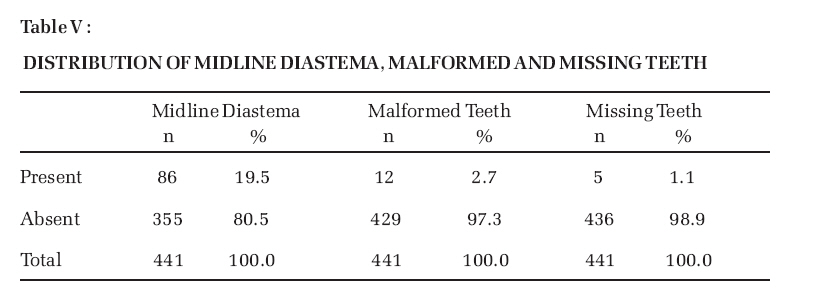
College of Medical Sciences, University of Benin, Benin City, Nigeria. Code Number: jm08009 ABSTRACT The aim of this study was to assess the prevalence of malocclusion in Benin City. A total of 441 school children, 229 males and 212 females of mean age 13.52 years ± 1.83 who had no previous history of orthodontic treatment were assessed for occlusal, space and dental anomalies. Angle's classification was used to assess buccal sagittal relationships. The results showed that 15.9% of the subjects had normal occlusion, 80.7% had Angle's class I and 1.1% had Angle's class II div 1, 0.5% had Angle's class II div 2 and 1.8% Angle's class III malocclusion. Increased overjet and overbite was observed in 24.7% and 9.8% respectively. Anterior open bite was present in 4.1% while crossbite was found anteriorly and posteriorly in 7% and 4.5% respectively. Crowding in the upper (11.1%) and lower anterior segment (12%) were similar while spacing was more prevalent in the upper (29.9%) than the lower anterior segment (10.7%) with midline diastema present in 19.5%. The occlusal traits were not influenced by gender difference (P>0.05). The survey revealed predominance of Class I malocclusion among Nigerian children in Benin City with their occlusal traits comparable to those reported from other Nigerian geo-political regions. KEYWORDS: Prevalence, Malocclusion, Nigerian children, Benin City INTRODUCTION The evaluation of the prevalence of different types of malocclusions existing within a population is important in order to plan orthodontic measures and determine the resources required for the services. A large number of epidemiological studies have been carried out to determine the prevalence of malocclusion in different racial and ethnic groups and the reported incidences varied in different populations1-5 . Some of these variations were attributed to the differences for specific ethnic groups and also the possible influences of registration methods of malocclusion trait and sample composition1 The earliest publications on the distribution of malocclusion in Nigeria were by Richardson and Ana6 , and Isiekwe and Logan7 which were clinic based. Several epidemiological surveys were further carried out to determine prevalence of malocclusion among Nigerian children and adolescents.8-10 Some of the studies reported the distribution of various classes of malocclusion in the Nigerian major ethnic groups of Yoruba11,12 and Igbo13 in South-Western and Eastern Nigeria respectively and Hausa14 in Northern Nigeria. These studies reported prevalence of normal occlusion in less than a third of Nigerian children and predominance of class I molar occlusal relationship. Presently, there is dearth of information in the literature on the prevalence of malocclusion in the South-Southern region of Nigeria in general and most particularly among school population in Benin City who are of age range that could avail themselves of orthodontic services. Therefore, the aim of this study was to determine the prevalence of malocclusion among school children in Benin City that would provide base-line data for the planning of orthodontic services and treatment measures on a population basis in this region of Nigeria. MATERIALS AND METHODS A sample of 441 children, 229 males (52%) and 212 females (48%) aged 11-18 years old with a mean age of 13 years ± 1.8 was randomly selected in four secondary schools from the list of one hundred and eighty five secondary schools in Benin City during the 2005 and 2006 academic session . The schools selected included public and private schools in order to have subjects from wide socio-economic class. The subjects were asked to indicate their state of origin to ensure their parents were of Southern Nigerian ancestry. None of the children had received any form of orthodontic treatment previously. Authorisation was sought and obtained from the schools' administrators and the parents who agreed to have their children examined gave informed consent.The author performed all the clinical examinations of the children in their classroom utilising mouth mirror, wooden spatula and a millimeter ruler with illumination provided by natural light. The children were examined for occlusal traits which included the occlusal antero-posterior relationship, overjet, overbite, openbite, crossbite, spacing, crowding, midline diastema and anomalies of missing permanent teeth, impacted / unerupted teeth and malformed teeth. Angle's classification15 was used to assess the buccal sagittal anteroposterior relationship of the upper and lower dental arches. Assessment was made on canines where first molars were missing. Overjet was defined as the horizontal measurement between the labio-incisal edge of the most prominent maxillary central incisors to the labial surface of the corresponding mandibular central incisors. It was measured with a millimeter ruler and evaluated to the nearest 0.5mm. An overjet value greater than 3.5mm was considered to be increased and less than 1mm to be reduced. The overjet was considered to be reversed when the maxillary central incisors were biting in lingual occlusion, which were further described as anterior crossbite. Overbite which is the vertical relationship of the upper and lower incisors was recorded as normal when the degree of overlap of the maxillary central incisors was between one third and one half of the clinical crown of the mandibular central incisors. The overbite was considered increased when the degree of overlap of maxillary central incisors was greater than one half of the clinical crown of the mandibular central incisors and reduced if the degree of overlap was less than one third. An edge to edge incisor relationship was recorded when the maxillary and mandibular incisors occluded on their incisal edges. Anterior open bite was recorded when incisal edges of the maxillary incisors did not overlap the incisal edges of the mandibular incisors. Posterior crossbite was considered lingual when the buccal cusp of the upper tooth occluded lingual to the maximum height of the buccal cusp of the opposing lower tooth. Buccal posterior crossbite (scissors bite) was recorded when the lingual cusp of the upper tooth occluded buccal to the maximum height of the buccal cusp of the opposing lower tooth. Crowding was defined as overlapping of erupted teeth as a result of insufficient space or lack of space for teeth to erupt in a segment. Spacing was recorded to be present when there was no approximal contact between teeth in a range of 1mm or more within a segment. Maxillary median diastema was recorded when a space of 2mm or more existed between the maxillary central incisors. Missing permanent teeth was registered when a permanent tooth that should have been erupted considering the subject's dental development was missing in the mouth. Malformed tooth was recorded for any erupted incisor of abnormal size or shape whose mesiodistal width was reduced or increased by 2mm or more. The intra-examiner reproducibility was assessed by re-examination of twenty five randomly selected school children two weeks after their initial examination. The data entry and analysis were carried out using IBM-compatible computer and Statistical Package for Social Sciences software version 11 (SPSS, Chicago, III). Statistical significance between frequencies and gender differences were evaluated with the chi-square test and p<0.05 was regarded as significant. RESULTS There was no statistically significant difference observed for any occlusal traits between the males and females (P > 0.05). Therefore, the combined data were analysed and Table I shows Angle's class 1 malocclusion had the highest frequency of 80.7% while other classes were rare. The normal overbite and overjet values were frequent findings with nearly a quarter had increased overjet (Table II). Anterior open bite was present in 4.1% while anterior and posterior crossbite was found in 7% and 4.5% of the subjects respectively (Table III). A normal dentoalveolar relationship predominates in the upper and lower arches with frequencies of 60.0% and 77.3% respectively as shown in Table IV. The frequency of crowding in both arches was similar while 29.9% had spacing of upper anterior segment and 10.7% had spaced lower anterior segment. Table V shows the presence of midline diastema in 19.5% of the subjects and malformed teeth in 2.7% and 1.1% with missing teeth. The reliability of the examiner was satisfactory with the kappa value of 0.92 indicating almost perfect agreement.16 DISCUSSION The prevalence of normal occlusion was 15.9% in this study and other classes of occlusion constituted 84.1% of which Angle's class I malocclusion was most predominant at 80.7%. The frequency of normal occlusion was higher than 12.2% observed in children of Northern Nigerian14 but lower than the findings of 24.4% and 27% reported among the children from south-western and eastern Nigerian12, 13 respectively. The predominance of Angle's class I malocclusion in this study was consistent with the previous reports from Nigerian populations but the frequency of 80.7% obtained was however higher than rates reported by Isiekwe 8 61.5%, Ogunbanjo13 65.5% and Onyeaso 12 50.0% in the previous surveys carried out in Southern Nigeria. These differences could be attributed to influences of registration methods, sample selection and possibly ethnic variation in occlusal and facial features. Similarly, high prevalence of class I malocclusion were also reported among surveys of African17-19 and African-American children.20 There was low prevalence of Angle's class II division 1 and division 2 malocclusions in this study which was consistent with findings of 1.7% in northern Nigerian children by DaCosta14 and studies from other parts of Africa 5,17,18 which also reported lower frequency of class II malocclusion when compared to higher prevalence rates of 8.2%, 12.3% and 27.2% observed in British populations.21-23 The frequency of Angle's class III malocclusion of 1.8% was also consistent with the low prevalence reported in Nigerian children and similar to findings of 1% in Tanzanian children17 . The normal overjet values were frequent findings in Nigerian children and high prevalence of 68.3% was also observed in this study while about a quarter of the subjects had increased overjet. A similar frequency of 65.7% was also reported among Yoruba adolescents 12. Isiekwe24 also reported prevalence of 58% and he attributed high prevalence of normal overjet values in Nigerians to the possibility of bimaxillary protrusion which is prevalent in Black race. A high prevalence of normal overbite was also observed which was consistent with other Nigerian studies.8,11-14 Also, 9.8% of the children had deep overbite and 8.4% had reduced overbite, 2% of which had edge to edge incisor relationship. The other vertical anomalies evaluated in this study included anterior open bite which was found in 4.1% of the school children while 7.0% of the children had anterior crossbite. Posterior crossbite was found in 4.5% of the subjects and both the lingual and buccal (scissor) crossbite were evenly distributed. There was a preponderance of normal dentoalveolar relationship in the upper and lower arches. Crowding in both the upper and lower anterior segment were comparable with frequencies of 11.1% and 12% respectively while spacing was more prevalent in the upper anterior segment (29.9%) than the lower anterior segment (10.7%). Midline diastema was observed in 19.5% of the children and similar to 17% reported by Isiekwe 25 while twice this incidence was reported by Onyeaso 12 in sample of south-western Nigerian children possibly due to influences of registration method. A high proportion of midline diastema observed was due to abnormal labial frenal attachment and dentoalveolar disproportion in Nigerian children. In addition, midline diastema in adults who engaged in aesthetic mutilation by artificially creating gap in their dentition to enhance beauty has been reported 25 . Frequently missing teeth was the maxillary lateral incisors which also constituted 75% of the malformed and microdontic teeth. CONCLUSION This study revealed predominance of Class I malocclusion among the children of the south-southern region of Nigeria. Normal overjet, overbite and dentoalveolar relationship were frequent findings with spacing of the upper anterior segment more common than crowding. No statistically significant gender difference was observed for any occlusal traits evaluated in this survey. References
© Copyright 2008 - CMS UNIBEN JMBR The following images related to this document are available:Photo images[jm08009t4.jpg] [jm08009t1.jpg] [jm08009t5.jpg] [jm08009t3.jpg] [jm08009t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}