 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 1, January-March, 2000, pp. 3-8 Study of Takayasu's Arteritis in Children: Clinical Profile and Management Muranjan MN, Bavdekar SB, More V, Deshmukh H*, Tripathi M, Vaswani R Departments of Paediatrics and Radiology*, Seth G. S. Medical College
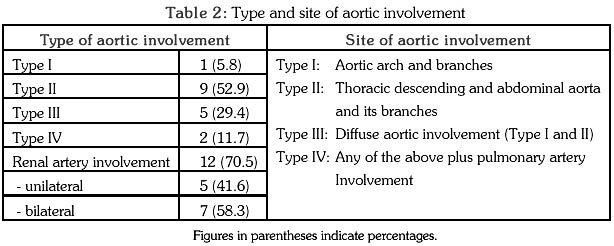
and K. E. M. Hospital, Parel, Mumbai - 400 012, India Code Number: jp00002 Abstract: AIMS: To study clinical features, pattern of involvement and treatment modalities of Takayasu's arteritis (TA) in children. MATERIAL AND METHODs: Retrospective analysis of hospital records of children admitted over a period of 4.5 years. Results: 17patients in the age group of 5 to 11 years (M: F = 1.1: 1) were diagnosed to have TA on the basis of Ishikawa's criteria. One child was diagnosed post-mortem. The commonest presenting features were hypertension (64.7%), congestive cardiac failure (47%), weak or absent peripheral pulses, cardiomyopathy (41.1% each) and cardiac valvular affection (35.2%). Retinopathy, hypertensive encephalopathy and abdominal bruits were uncommon. None presented in the prepulseless phase. No patient had an active tuberculous lesion, although Mantoux or BCG test was positive in 6 (35.2%). The predominant pattern of angiographic affection was Type II (52.9%). Nephrotic syndrome and portal cavernoma seen in one patient each were incidental associations. Anti-hypertensive drugs, oral steroids and drugs to control congestive heart failure were the mainstays of medical management. Antitubercular therapy was started in six patients. Angioplasty was attempted in 15 cases and proved to be partially beneficial in six. Three patients who failed to respond to medical management had to undergo surgical procedures, either bypass, nephrectomy or both. In-hospital mortality was 11.7%. Conclusions:of TA in this study presented acutely in the pulseless phase, with hypertension and its complications. Type II involvement was the commonest pattern. Anti-hypertensive agents and steroids along with angioplasty were partially successful in controlling symptoms in 35.2%. Surgical procedures were reserved for a minority with poor response to drugs and angioplasty. (J Postgrad Med 2000; 46:3-8) Key Words: Takayasu's arteritis, Non-specific aortoarteritis, Childhood hypertension Takayasu's arteritis (TA) is the commonest acquired disorder of the aorta and its branches. Its aetiopathogenesis remains a subject of speculation even 90 years after it was first described by the Japanese ophthalmologist, Takayasu. Initially, cases were reported predominantly from Japan, Southeast Asia and Africa 1,2 . It is now being recognized as a disease with a worldwide distribution 3 . It is commonly described as a disease of young women, affecting them in the second or third decades. The clinical features of TA are said to be different in the paediatric and adult age groups. A study was undertaken to analyse the clinical profile and management strategies employed in managing children with TA. Material and Methods Hospital records of children admitted to a large tertiary care centre between January 1995 and April 1999 were reviewed. Demographic data, presenting features, clinical findings, results of investigations carried out and treatment modalities employed were recorded in a proforma and the results were analysed. Ishikawa's criteria 4 were used to establish the diagnosis of TA while NIH criteria were followed for ascertaining disease activity 5 . Aortic involvement was classified on the basis of Lupi - Herrera's modified classification 6 . Results During the study period, 17 patients (9 boys, M : F = 1.1:1) aged 5 to 11 years were admitted in the hospital with TA. The mean age at presentation was 9.3 years. As shown in Table 1, hypertension and its complications formed the predominant presenting manifestations. No patient had active tuberculous lesion, although Mantoux or BCG test was positive in 6 (35.2%). Anti-streptolysin O (ASO) and anti-nuclear antibody (ANA) titres were elevated in 1 child each without clinical features of rheumatic or autoimmune disease. One child presented with clinical and biochemical features of Nephrotic syndrome in whom kidney biopsy revealed acute diffuse endocapillary glomerulonephritis. Another patient was noted to have an asymptomatic portal cavernoma on abdominal ultrasonography. A 9 years old boy who had undergone mitral valve replacement for rheumatic mitral regurgitation presented with sudden cardiac failure. Post-mortem examination including histopathological studies of aortic tissue suggested a diagnosis of TA. Except for the child in whom TA was diagnosed post-mortem, the diagnosis and extent of involvement was determined on the basis of aortic angiography and classified on the basis of Lupi - Herrera's modified classification 6 . Type II involvement was determined to be the commonest pattern (Table 2). Pulmonary perfusion scintigraphy could be carried out in only two children, both of whom showed unilateral involvement of segmental pulmonary arteries. Anti-hypertensive drugs were started in all 13 patients who presented with hypertension. All of them required at least 3 anti-hypertensive agents for controlling the blood pressure initially. Ten subjects (58.8%) had active disease and were started on oral prednisolone in a daily dose of 1-2 mg/kg-body weight. Percutaneous transluminal angioplasty (PCTA) was performed in 15 subjects after control of ESR. The procedure was technically successful in all 15 patients. In six subjects (40%) the procedure was partially successful, but complete success with total withdrawal of anti-hypertensive drugs could not be achieved in any. Placement of a stent in the abdominal aorta was attempted in one, but the stent could not be negotiated due to severe luminal narrowing. Two patients each underwent nephrectomy or iliorenal bypass, while both procedures were performed in one subject (Figs. 1, 2, 3, 4). The overall in-hospital mortality was (11.7%). Discussion TA is the commonest cause of renovascular hypertension in Asians and Africans 7 . The disease is described to have 3 types of presentations 3,8 . In the prepulseless phase the manifestations are non-specific and include malaise, fever, headache, arthralgia, myalgia and weight loss. Angiodynia is a feature of the second phase during which the patient experiences pain along the affected vessels. Hypertension, pulselessness and complications of hypertension characterize the third phase. All our patients had these manifestations, which could be due to physicians being unable to recognize the disease in the prepulseless phase. It is also possible that in our population these early manifestations are non-existent or too mild for parents to seek medical attention for. It is important to recognize the disease at an early stage as clinical and angiographic improvement has been achieved by early institution of immunosuppressive therapy and progressive arterial changes can be reversed or prevented 9,10 . Certain manifestations of TA such as fever, arthralgia, cardiac failure and elevated levels of acute phase reactants are similar to those of rheumatic fever 1,3,11 . Regurgitant murmurs of the mitral and aortic valve have been reported in 11% and 55% of cases with TA 3 respectively. This could lead to misdiagnosis in developing countries with a high prevalence of rheumatic fever. In our series, one of the patients was on secondary prophylaxis against rheumatic fever and was diagnosed to have TA post-mortem. A high index of suspicion, proper evaluation of non-specific complaints, meticulous examination of all peripheral pulses and recording of blood pressure in all four limbs would aid in early diagnosis of TA in children. Several differences have been observed between paediatric TA and adult disease. An increased frequency of constitutional symptoms noted in children could account for delayed diagnosis. Other authors describe acute symptoms due to hypertension and its complication to be the predominant manifestations in children resulting in shorter interval before diagnosis. This was also reflected in our series where congestive heart failure and encephalopathy secondary to hypertension were the major manifestations. Symptoms due to limb and CNS ischaemia, which are frequent in adults, are seldom reported in children. Only one case in our series had a neurologic deficit, but that too was secondary to hypertensive encephalopathy. None of the children in our series complained of symptoms attributable to limb ischaemia, even though poor or absent pulses were clinically evident. Abdominal and thoracic segments of the aorta are preferentially affected in children and symptoms due to this pattern of involvement can mimic coarctation of aorta. Aneurysm formation commonly encountered in adult TA is rare in children, though aneurysms in paediatric TA have been reported from India 1,3,12 . Given the heterogeneity of the disease depending upon geographic location, it is not surprising that none of the criteria enjoy universal applicability. Ishikawa's criteria 4 and those of the American College of Rheumatology 13 tend to underdiagnose TA in the Indian population. Indians, as demonstrated in our study have a predominant involvement of thoracic and abdominal aorta. Hence, Sharma et al 14 have suggested certain modifications for increasing the sensitivity of the diagnostic criteria. The aetiopathogenesis of the disease remains enigmatic. Tuberculosis was proposed to be one of the predisposing factors. In our series, none of the children had an active tubercular lesion and cutaneous hypersensitivity to tubercular protein could be noted in only 35.2% of cases. Tuberculosis being highly prevalent in India, it is possible that early studies may have found associated tubercular lesions in many cases of TA 15,16 . Various mechanisms such as post-autoimmune, ethnic susceptibility and a genetic predisposition have been evoked. Autoimmunity appears to be the most plausible mechanism 3 . Both cellular and humoral factors are probably involved. Defective T lymphocyte regulation and anti-endothelial antibodies have been implicated. A provocative hypothesis put forward by Kothari 17 explores the possibility of BCG vaccination as a triggering factor for TA in a susceptible population. A 65 M heat shock protein (HSP) that plays a role in vascular injury has been shown to be a component of both BCG and Mycobacterium tuberculosis. The diagnosis is established and the extent determined with the help of angiographic studies, although Doppler could indicate the diagnosis in some. TA has been known to involve pulmonary artery as well and this affection can be picked up on the basis of MRI or radionuclide perfusion scans 18 . The disease activity has conventionally been decided upon on the basis of raised ESR, although presence of fever, pain of vascular origin and elevated C-reactive protein could be additional criteria that may indicate active disease 19 . Besides management of hypertension and its complications, steroids and immunosuppressive agents like methotrexate and cyclophosphamide are used to suppress disease activity 3,5,19 . Response to therapy is faster and better in children with a higher rate of remission, though other authors have documented an aggressive course of juvenile TA 1 . Our patient population had fibrotic arterial disease but had some disease activity as could be seen from the fact that most had an elevated ESR. Fortunately, they responded to steroid therapy. Other components of medical therapy include anti-platelet agents like aspirin and dipyridamole, which have been used especially in patients with transient neurological symptoms. Role of intravenous immunoglobulins, recombinant IL-1 receptor antagonists, IL-4 and transforming growth factor b is yet to be established 3 . Interventional radiological techniques have provided a viable and less invasive alternative to surgery. Percutaneous transluminal angioplasty (PCTA) is the commonest palliative procedure performed with a success rate varying from 56 - 80% 3,5,20 . The procedure can be carried out at the time of angiography itself Flank pain during the procedure is the commonest side effect. Dissection, pseudoaneurysm or creation of an intimal flap are the rarely encountered complications of this procedure. Re-stenosis can occur 3 . Placement of a self-expanding stent has been carried out successfully in adults but is technically difficult to perform in children, given the small calibre of vessels. All lesions are not amenable to PCTA and surgical bypass procedures become imperative when stenosis exceeds 70%. Although, it is recommended that such procedures be delayed in children, at least till their growth is complete; splenorenal shunting has been undertaken in a two-year-old child 21 and splenorenal and aortorenal bypass have been successfully carried out in children 7 . Irrespective of the surgical procedure undertaken, the outcome appears to be favourable when the disease is quiescent 22,23 . Acknowledgement The authors thank The Dean Seth G. S. Medical College and K. E. M. Hospital for granting permission to publish this article. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00002f1.jpg] [jp00002f4.jpg] [jp00002t1.jpg] [jp00002f2.jpg] [jp00002t3.jpg] [jp00002f3.jpg] [jp00002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}