 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
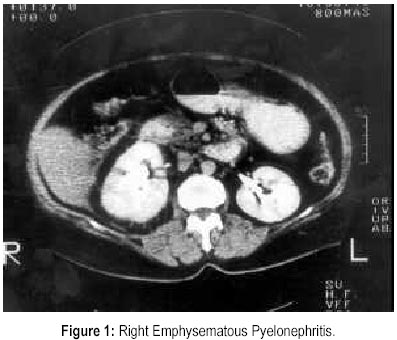
Journal of Postgraduate Medicine, Vol. 46, No. 1, January-March, 2000, pp. 31-32 Case Report Emphysematous Pyelonephritis: A Rare Presentation Jain SK, Agarwal N, Chaturvedi SK* Departments of Medicine and Radiology*, Dr. Ram
Manohar Lohia Hospital, New Delhi - 110001, India Code Number: jp00009 Abstract: Emphysematous pyelonephritis is a rare life threatening infection in diabetes characterised by suppurative infection of renal parenchyma and perirenal tissues. It usually presents with fever, nausea, vomiting, abdominal pain, shock, lethargy, and confusion. Diabetic ketoacidosis is an uncommon presentation. In the present case, an elderly female presented with abdominal pain, fever, vomiting, and altered sensorium. She was diagnosed to have diabetic ketoacidosis with metabolic encephalopathy with right emphysematous pyelonephritis. She had an excellent response to medical treatment alone and was later discharged on oral hypoglycaemic agents. (J Postgrad Med 2000; 46:31-32) Key Words: Diabetes, Ketoacidosis, Metabolic Encephalopathy, Pyelonephritis, Emphysematous. Emphysematous pyelonephritis is a rare life threatening, suppurative infection of renal parenchyma and perirenal tissues. It is seen mostly in diabetic patients in association with urinary tract obstruction. Clinical features are fever (56%), nausea, vomiting (16%), abdominal pain (7%), shock (16%), lethargy and confusion (24%) 1 . Diabetic ketoacidosis is very uncommon 1 . Case Report A fifty year old female presented with dull continuous pain in right upper abdomen, fever and vomiting for four days followed by altered sensorium and seizures for a day. On examination patient was febrile, disoriented with pulse rate of 110 per minute, blood pressure of 130/180 mm of mercury and respiratory rate of 28 per minute. Chest and heart examination were normal. On abdominal examination, there was tenderness in right hypochondrium and lumbar region and sluggish bowel sounds. There were no meningeal signs or focal neurological deficit. Investigations revealed haemoglobin of 12.5 g per dl, total leucocyte count of 7000 per cubic mm, differential leucocyte count of 77% neutrophils, 21 % lymphocytes and 2% eosinophils, erythrocyte sedimentation rate of 130 mm in first hour, blood sugar of 250 mg per dl, blood urea of 40 mg per dl, serum creatinine of 0.7 mg per dl, serum sodium of 133 mEq per litre, serum potassium of 2.8 mEq per litre and urine ketones were 2+. Arterial blood gas analysis revealed metabolic acidosis. Blood and urine culture were sterile and urine microscopic examination showed 8-10 pus cells per high power field. Chest roentgenogram was normal. Abdominal ultrasonography (USG) showed right hydronephrosis and dilated bowel loops. Intravenous pyelography (IVP) showed non-obstructive hydronephrosis with normal excretory function of kidneys. Contrast enhanced computerised tomography (CECT) of abdomen showed right emphysematous pyelonephritis with normal excretion of contrast on both sides (Fig. 1). Patient was therefore diagnosed as a case of diabetic ketoacidosis with metabolic toxic encephalopathy with right emphysematous pyelonephritis and managed with plain insulin infusion, potassium supplementation, injectable ceftazidime and netilmycin. Patient started improving after three days with complete resolution of signs and symptoms in ten days. Antibiotics were however continued for 15 days and repeat USG and CECT abdomen were normal. Discussion This is an interesting rare case of emphysematous pyelonephritis presenting as diabetic ketoacidosis of which only one case has been reported so far in a 17-year-old girl 2 . Diagnostic sensitivity of IVP and USG of abdomen are 50% and 85% respectively 1,3 . In the present case, both the investigations failed to clinch the diagnosis until CECT abdomen was done which is 100% sensitive. Non-obstructive hydronephrosis observed on USG and IVP which resolved after treatment denotes loss of peristalsis due to endotoxin secondary to infection which reverses after infection is treated. It is seen only in 15% of cases 4,5 . Besides high mortality of 75% is observed with medical treatment in contrast to 11% with surgical treatment and 7% with combined treatment in a case of emphysematous pyelonephritis 1 . In our case, patient started improving in 3 days thus precluding surgical treatment which is very unusual. To conclude, although emphysematous pyelonephritis is a rare and life threatening condition, a timely diagnosis and intensive early management can not only thwart nephrectomy and decrease morbidity but mortality also. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00009f1.jpg] |
| |||||||||

{kind=link}