 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 1, January-March, 2000, pp. 35-36 Case Report Active Contrast Extravasation In Spontaneous Rupture Of Hepatocellular Carcinoma: A Rare CT Finding Rathod K, Sheth R, Shah P, Rege S* Departments of Radiology and Surgery*, Seth
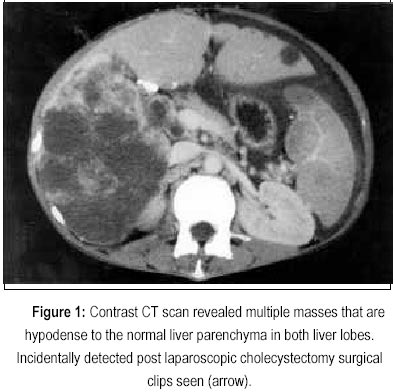
G. S. Medical College and K. E. M. Hospital, Parel, Mumbai - 400 012, India. Code Number: jp00011 Abstract: Spontaneous rupture of hepatocellular carcinomas are uncommon but constitute a critical and life threatening condition. Diagnosis is important so that either surgery or emergency arterial embolisation can be considered for hepatic haemostasis. We describe active extravasation of intravenous contrast medium on CT in a patient who presented with intraperitoneal haemorrhage secondary to spontaneous rupture of hepatocellular carcinoma. (J Postgrad Med 2000; 46:35-36). Key Words: Hepatocellular Carcinoma, Spontaneous rupture, Intravenous Contrast, CT. Spontaneous rupture of hepatocellular carcinoma (HCC) is uncommon. Intraperitoneal rupture of HCC may be demonstrated by computed tomography (CT) as high density ascites adjacent to peripheral mass 1 . High density ascites on CT has also been descried in excessive anticoagulation, following abdominal trauma, spontaneous rupture if other abdominal neoplasms including hepatic adenomas, cavernous haemangiomas, or angiosarcoma. However, in spontaneous rupture of HCC, CT finding of intraperitoneal extravasation of intravenous contrast is very rare. Case Report A 42-year old woman presented with acute abdomen, distension and dyspnoea. Over last three months, she had developed abdominal pain, weight loss and asthenia. She had undergone laparoscopic cholestectomy six months ago. Clinical examination revealed tachycardia, pallor, hypotension and hepatomegaly. Abdominal tap revealed blood. CT-Computed Tomography Abdomen performed without oral contrast with intravenous (IV) contrast revealed multiple hypodense lesions scattered in the liver (Fig. 1); active intravenous contrast extravasation in the perisplenic region (Fig. 2), high density ascites, lymphadenopathy and splenic infarcts. Patient expired after two days. Post-mortem examination revealed haemorrhagic fluid in the peritoneal cavity; hepatomegaly with multiple white nodules with haemorrhagic foci within them and abdominal lymphadenopathy. Histologic diagnosis of the liver lesion revealed hepatocelullar carcinoma. Discussion Spontaneous rupture of hepatocellular carcinoma occurs in 10% of patients 1 and accounts for 10% of deaths in patients. Hepatocellular carcinomas are apt to undergo central degeneration and haemorrhage rupture of a peripherally situated mass causes haemoperitoneum. The mechanism postulated is progressive or sudden occlusion of the draining veins by the tumour (either by compression from tumour growth or invasion), increase in pressure within the tumour and rupture occurring at the surface 2 . Increased tumour size and extent of extrahepatic protrusion are associated with increased risk of hepatocellular rupture 1 , which can be diagnosed on CT. A high tumour protrusion ratio, high density ascites adjacent to tumour, elevated ascitic CT numbers, number of involved liver segments, maximum tumour area, are important CT findings indicating hepatocellular rupture. The maximum length of protrusion, calculated on CT by measuring the maximal length of the most protruded margin on the CT scan 1,4 . CT studies show a peripheral hepatic tumour and a large amount of free intraperitoneal fluid with areas of high attenuation representing acute blood clot 5 . CT findings in the illustrated case shows a peripheral hepatic tumour and a large amount of intraperitoneal fluid with areas of high attenuation and active IV contrast extravasation, as a rare CT finding, which illustrates the value of CT in establishing the diagnosis of spontaneous rupture. Pre-treatment transfemoral angiography have shown active extravasation of contrast 3 . Prognosis of spontaneous rupture is poor and these patients are poor surgical candidates because of cirrhosis and extensive tumour replacement of the liver and carries a high risk of morbidity and mortality. However, it is found that transcatheter hepatic artery embolisation is an effective therapeutic procedure in ruptured hepatocellular carcinoma, achieving in some patients 15 months survival 3 . Therefore, it is essential that early detection of the findings described on CT is essential for immediate intervention. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00011f1.jpg] [jp00011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}