 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 1, January-March, 2000, pp. 37-38 Case Report Round Worm Migration Along Ventriculoperitoneal Shunt Tract: A Rare Complication Agarwal P, Malapure SM, Gupta R, Mane P, Parelkar S, Oak SN Department of Paediatric
Surgery, T. N. Medical College and B. Y. L. Nair Ch. Hospital, Mumbai - 400 008,
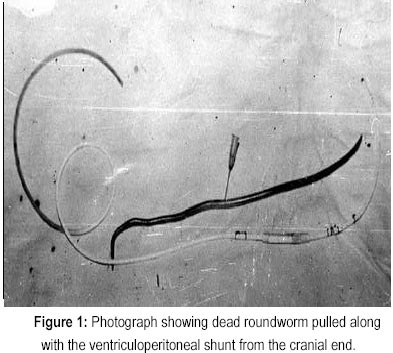
India. Code Number: jp00012 Abstract: Though a ventriculoperitoneal shunt has been associated with myriads of unusual complications, so has been that with roundworms. A case of a three-year-old boy is presented who had an unusual complication of roundworm migration along the shunt tract that presented as shunt tract infection. (J Postgrad Med 2000; 46:37-38) Key Words: Ventriculoperitoneal shunt, Complication, Ascariasis. The common complications associated with ventriculo-peritoneal (VP) shunts are obstruction, shunt infection ventriculitis and shunt migration, etc 1 . Unusual complications include complete migration of the VP shunt into the ventricle or even passage through the rectum 1,2 . On similar lines, symptomatology commonly encountered by a paediatric surgeon related to roundworm infestation are obstruction (due to bolus formation or intussusception), perforation (due to penetration of ulcers) or retrograde migration to stomach and upper aero-digestive tracts. Infrequent complications include appendicitis, obstructive jaundice, pancreatitis, liver abscesses and obstructions at anastomotic sites 3,4,5 . The above features are due to the tendency of the roundworms to negotiate small orifices, which serves as an impetus for further migration 6 . Case Report A three-year-old boy presented with high-grade fever and redness of right mastoid region of five days duration. He was mentally retarded with delayed milestones. The patient was treated for tubercular meningitis with hydrocephalus, for which a VP shunt was introduced when the patient was a year old. He made uneventful recovery after the surgery till the present illness. There was no history of abdominal discomfort or any respiratory problems in the past. There was history of passage of roundworms in the stools on three occasions and he had vomited a roundworm once. On local examination, there was redness over the mastoid area and mastoid tenderness was present. Shunt was functioning and skin over the tract was inflamed. Abdominal wound was unhealthy and on milking the shunt tract, pus could be expressed through the abdominal wound. Pus was sent for culture and sensitivity. The patient was started on vancomycin and amikacin. Despite five day antibiotic therapy, there were no signs of resolution Therefore; it was decided to remove the shunt. Under local anaesthesia, a small incision was given over the previous cranial incision and the shunt was removed. While removing the shunt a membranous soft tissue was pulled along the tube, which was thought to be a necrotic fascia around the shunt. On full withdrawal of shunt, the soft tissue was found to be a dead roundworm. The wound was stitched and shunt tip was sent for culture and sensitivity. The patient was on antibiotics for 15 days after which a fresh shunt was introduced on the opposite side when all infective foci had disappeared. Discussion Infection remains the foremost complication associated with shunt procedures for hydrocephalus. Many studies emphasize the frequency of shunt infections in either ventriculo-atrial or VP shunts. The factors responsible for shunt infections are poor preoperative skin conditions, intercurrent seats of infection, patient's age, type of operation (whether primary insertion, revision, or reinsertion after infection), which end of the shunt was revised and the presence of post operative wound dehiscence or scalp necrosis 7 . Though Staphylococcal epidermidis was the most common pathogen along with other gram negative and gram positive pathogens we could not find a similar case report as ours where a roundworm had migrated along the shunt track and was the cause of shunt tract infection. It was unusual regarding the migration of roundworm from the bowel lumen without demonstrable signs of perforative peritonitis. In some instances, several roundworms may be found lying free in the peritoneal cavity in absence of a demonstrable perforation in the intestinal wall 8 . Roundworm migration has been reported through the umbilicus and the drainage tube of an empyema 9,10 . Roundworms are also seen coming out of infected inguinal wound following strangulated hernia repair and from drainage site of a subphrenic abscess 11,12 . Roundworms on rare occasion migrate far out from the gastro intestinal tract and are located in place like pleural cavity, lacrymal duct, middle ear and even in femoral artery. Round worm have been reported to have caused fatal invasion of the pelvis of the left kidney through a uretero colic fistula 13,14 . We present this unique case report for its rarity and claim it to be the first of its kind as there is no mention of a similar case report in the literature. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00012f1.jpg] |
| |||||||||

{kind=link}