 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 75-79 The Palm Print as a Sensitive Predictor of Difficult Laryngoscopy in Diabetics: A Comparison with Other Airway Evaluation Indices Vani V, Kamath SK, Naik LD Department of Anaesthesiology, Seth G. S. Medical College and K .E.
M Hospital, Parel, Mumbai-400012, India. Code Number: jp00020 Abstract AIMS: To evaluate the ink impression made by the palm of the dominant hand as a screening tool for difficult laryngoscopy in diabetic patients. SUBJECTS AND METHODS: In this prospective study, airway of 50 adult diabetic patients, undergoing elective surgery under general anaesthesia, was assessed preoperatively using the common clinical indices such as Modified Mallampati test, thyromental distance, degree of head extension and a specific index- the palm print test. Following induction of anaesthesia and neuromuscular relaxation, laryngoscopy was performed and the laryngoscopic view scored. The sensitivity, specificity and positive predictive value of each airway evaluation index were calculated. RESULTS: The incidence of difficult laryngoscopy was 16%. The palm print test had the highest sensitivity (75%) of all the indices. The thyromental distance less than six cm had the highest specificity (95.2%) but was least sensitive (25%). 87% of patients with difficult laryngoscopy had two or more indices abnormal. CONCLUSION: Though the palm print test was the most sensitive index of the four indices studied, a better prediction of difficult laryngoscopy can be achieved by evaluating all the four airway indices preoperatively. (J Postgrad Med 2000; 46: 75-79) Key words: Diabetes, Difficult intubation, Palm print. Securing and maintaining an adequate airway is the fundamental responsibility of an anaesthetist. It has been estimated that inability to successfully manage difficult airway has been responsible for as many as 30% of deaths attributable to anaesthesia 1,2 . The incidence of difficult and failed intubation has been reported to be 1-3.6% and 0.05-0.3% respectively 3 . Preoperative identification of those patients at risk of difficult laryngoscopy therefore assumes importance in order to formulate an appropriate strategy for the induction of anaesthesia and the intubation. To anticipate difficult airway preoperatively, many clinical indices have been devised, the commonly used ones being the modified Mallampati test, the thyromental distance and the degree of head extension. Unfortunately, most of these have a low sensitivity and specificity 4-6 . By examining features specific to a sub-population of patients, improved sensitivity of the test may be achieved 3 . Fifty percent of the diabetic patients undergo surgery some time during their life 7 . The diabetic patients are particularly prone to difficult laryngoscopy and intubation, the reported incidence being 27-31% 3,8,9 . This is due to non-enzymatic glycosylation of collagen and its deposition in the joints resulting in 'Limited joint mobility' (LJM) syndrome, which occurs in 25-45% of patients with long standing diabetes 3,10 . Involvement of the atlanto-occipital joint limits adequate extension of head and neck during laryngoscopy leading to intubation difficulties 8,10,11 . These changes initially start in the fourth and fifth interphalangeal joints because of which the patient is not able to approximate the palms and fingers of the hands, the 'Prayer sign' 8 . The degree of the interphalangeal joint involvement can be objectively assessed by scoring the ink impression made by the palm of the dominant hand as proposed by Reissell et al 3,9 . The purpose of this study was to compare the sensitivity and specificity of the palm print test with the commonly used indices in their ability to predict difficult laryngoscopy in diabetic patients. Subjects and Methods Fifty adult diabetic patients undergoing elective surgery under general anaesthesia were studied. Following exclusion criteria were considered.
Preoperatively, airway was assessed in each patient while they were sitting upright in a chair using the modified Mallampati test, thyromental distance, degree of head extension and the palm print test. Scores were given for each index as follows: Modified Mallampati Test 12 : Keeping the head in neutral position the patient was asked to open the mouth fully and protrude the tongue as far as possible. Looking from the patient's eye level the pharyngeal structures were inspected with a torch without the patient phonating and the view was graded as follows:
Thyromental Distance 3 : The patient was asked to fully extend the neck from neutral position. The distance from the mentum to the thyroid notch was measured with a thread and a measuring scale and graded as
Distance ³ 6cm (Grade 0) is normal. Head extension 3 : Keeping the head in neutral position and the line joining the mentum to the angle of the mandible parallel to the floor, the patient was asked to maximally extend the head on the neck. The angle traversed by the mentomandibular line was measured using a protractor compass.
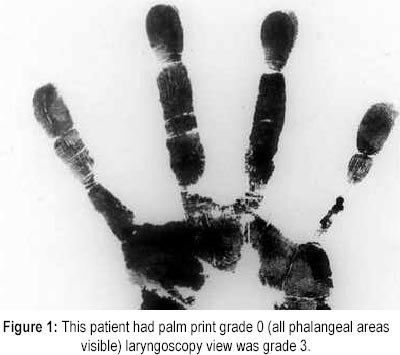
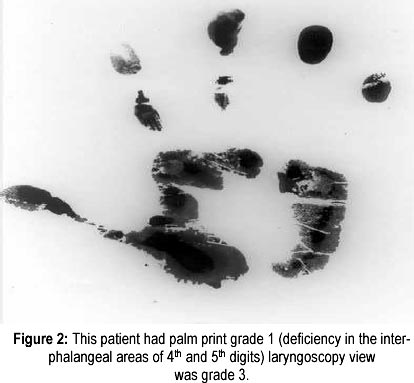
Head extension degree ³ 35 (Grade 0) is normal. Palm Print Test 3,9 : The palm and fingers of the dominant hand of the patient was painted with black writing ink using a brush. The patient then pressed the hand firmly against a white sheet of paper on a hard surface (Figures 1 and 2). Scoring was done as:
On presentation at the operating room, monitors were attached and after pre-oxygenation, general anaesthesia was induced with 2.5% thiopentone sodium 5 mg/kg and succinylcholine 2 mg/kg. After full muscle relaxation laryngoscopy was performed by a qualified anaesthetist using a Macintosh blade. The laryngoscopist tried up to 3 attempts to acquire the best laryngeal view without external laryngeal pressure applied to the cricoid cartilage. The laryngoscopist assigned a laryngeal view class based on the criteria of Cormack and Lehane 13 .
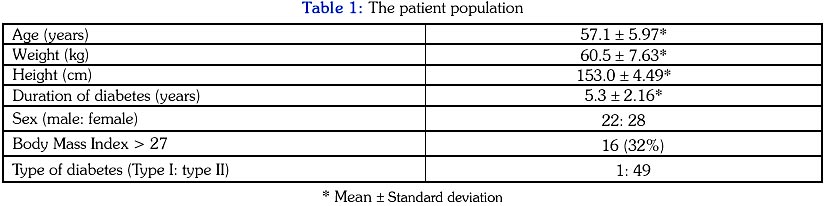
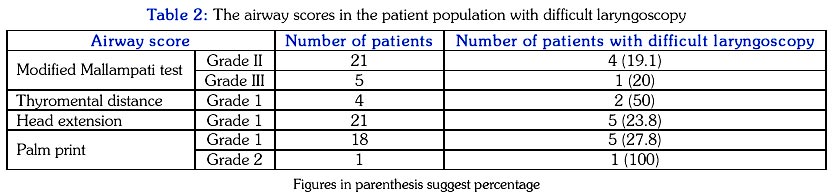
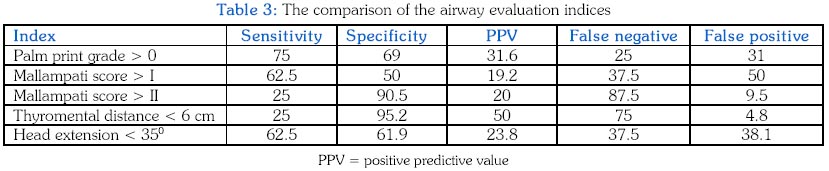
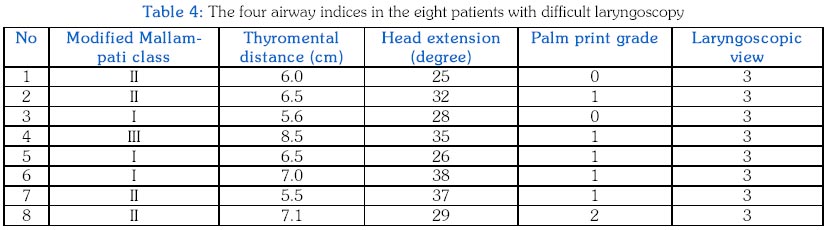
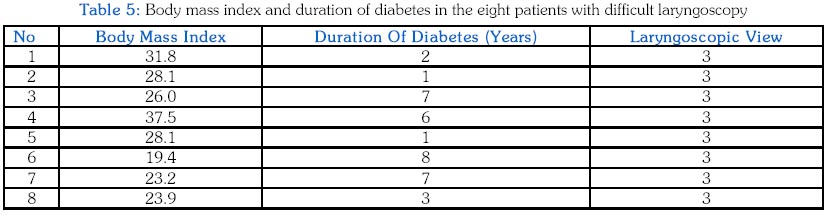
Grade III & IV laryngoscopic views are considered as difficult laryngoscopy as no part of the glottis is visible. After laryngeal view was graded, patient was intubated with appropriate sized endotracheal tube and the correct placement of the tube was confirmed. Stylet, gum elastic bougie and long Macintosh curved blade were kept ready and used when required. In order to compare the clinical performance of the four indices: sensitivity, specificity, positive predictive value, false negative and false positive ratios were calculated by simple 2 X 2 tables. Results The demographic data of the 50 diabetic patients is given in Table 1. The table 2 gives the details of various airway scores in the patient population. Sensitivity, specificity and positive predictive value were calculated for each index (Table 3). Eight patients had grade III laryngoscopic view, and no patient had grade IV view. The incidence of difficult laryngoscopy was therefore 16%. The details of these eight patients are given in the table 4. Four (50%) of the patients with difficult laryngoscopy were obese (Body mass index more than 27) 3 . The duration of diabetes in all the eight patients was less than 10 years and in four patients, it was less than five years (Table 5). Discussion Among the various endocrine disorders, diabetes mellitus is the commonest an anaesthetist encounters. Improved management of diabetes has resulted in an increase in the number of diabetic patients presenting for surgery both elective and emergency, many of them requiring general anaesthesia with tracheal intubation. Since the time Salzarulo et al 10 published their report on difficult laryngoscopy in a diabetic patient, there has been a growing interest in this problem. Studies by Hogan et al 8 , Reissell et al 9 and Nadal et al 3 have reported 32%, 31% and 27% incidence of difficult laryngoscopy respectively in diabetic patients. In our study the incidence was 16%. The lower incidence in our study could be because of the lower average duration of diabetes (5.3 years) as compared to 24 years and 10 years in studies by Reissell et al and Nadal et al respectively. Four airway indices were evaluated with respect to their ability to predict difficult laryngoscopy pre-operatively. The palm print test was found to have the highest sensitivity (75%) followed by head extension <35° and modified Mallampati grade >I; thyromental distance < 6 cm and modified Mallampati grade >II in that order (Table 3). Nadal et al 3 in a similar study have found the palm print to be 100% sensitive. The other three indices had lower sensitivity as compared to our study. In the study by Nadal et al duration of diabetes >10 years was found to be a sensitive indicator of difficult laryngoscopy, only two patients with duration less than 10 years had difficult laryngoscopy. However, in our study the duration of diabetes in all the patients in whom laryngoscopy was difficult had diabetes was less than 10 years and in 50% less than five years. Correlating all the four indices in the eight patients with difficult laryngoscopy, we found that in four patients, three of the four indices were abnormal; in three patients, two indices were abnormal and in one patient one index was abnormal (Table 4). Thus in seven out of eight patients (87%) two or more of the indices were abnormal. Thus by evaluating all the four airway indices, a better prediction of difficult laryngoscopy can be achieved. The increased incidence of difficult laryngoscopy in diabetic patients is thought to be due to development of LJM syndrome. The exact mechanism of LJM syndrome has not been elucidated. Existing evidence suggests that the syndrome may be another example of tissue glycosylation associated with chronic hyperglycaemia seen in diabetic patients 9,14 . Diabetic patients have an abnormality of collagen metabolism and increased cross-link formation as a result of which collagen fibrils are abnormally stable, relatively insoluble and resistant to enzymatic degradation 9,15 . These changes are potentially reversible 9,16 . Reissell et al 9 have speculated that glycosylation of the joints of larynx and cervical vertebral region may be responsible for the increased incidence of difficult intubation. The changes in the LJM syndrome usually begin in the metacarpophalangeal and proximal interphalangeal joints of the fifth finger and gradually extend medially as a result; the patient will not be able to approximate the palm and fingers of the hands 9,14 . The joint limitation is painless and non-disabling. No relationship has been found between the LJM syndrome and sex, race or control of diabetes 14 . The duration of diabetes and age attained are important variables in development of the LJM syndrome 14,17 . The LJM syndrome being a painless disorder with minimal disability is often unnoticed at the time of proposed surgery unless specifically looked for. A simple bedside test would be to observe the patient's hands for thick, waxy skin, placing the patient's hands in "prayer" position and assessing the degree of inability to oppose the interphalangeal joints of the fingers 8,9 . In this study, there was no relation between the duration of diabetes and difficult laryngoscopy. This could be because of the lower average duration of diabetes in our study. The palm print test was not evaluated in the non-diabetic population. Laryngoscopy view was used to evaluate the airway indices in our study. Although difficult laryngoscopy does not mirror difficult intubation, laryngoscopic view is an accepted method of comparing airway evaluation indices 18 . During induction of anaesthesia a false positive airway evaluation test may result in over-preparation and subject the patient to unnecessary procedure. Though undesirable, this is preferable to a false negative prediction, which may result in a disaster, particularly in a diabetic patient where diabetic motor dysfunction, residual gastric contents and hyperacidity increase the risk of pulmonary aspiration during induction of anaesthesia 9,19,20 . Rapid securing of the airway at the induction of anaesthesia is essential in patients at risk, making preoperative identification of the diabetics with difficult airway important. Use of the palm print should aid the anaesthetist to anticipate difficult laryngoscopy in diabetic patient. However, evaluation all the four airway indices offers a better prediction of difficult laryngoscopy and if two out of the four indices are abnormal one should prepare for difficult intubation. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00020t3.jpg] [jp00020f2.jpg] [jp00020f1.jpg] [jp00020t5.jpg] [jp00020t1.jpg] [jp00020t4.jpg] [jp00020t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}