 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 91-93 Case Report Scleredema Adultorum Parmar RC, Bavdekar SB, Bansal S, Doraiswamy A, Khambadkone S The
Department of Paediatrics, Seth G. S. Medical College and K. E. M. Hospital, Parel,
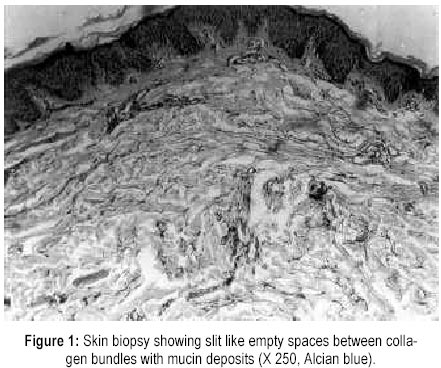
Mumbai - 400 012. Code Number: jp00024 Abstract: Scleredema adultorum is a rare connective tissue disorder reported usually following streptococcal infection, influenza, measles, and mumps. It has been reported occasionally following trauma and tuberculous lymphadenitis. This is a report of scleredema adultorum developing after chicken pox in an eight-year-old male child. The diagnosis was established by characteristic picture on skin biopsy using special stain. The patient had a benign course and a spontaneous recovery in two weeks. The case has been reported as the first case of scleredema adultorum developing after chicken pox. (J Postgrad Med 2000; 46:91-93) Key words: Scleredema, Varicella, Skin Biopsy, Dermis, Connective Tissue, Mucopolysaccharide, Collagen Scleredema adultorum is a rare connective tissue disorder of unknown aetiology. After its first description by Buschke et al in 1900, more than 300 cases have been reported so far. Although it has been well-described entity in the European medical and dermatological journals, very occasional cases have been reported from India. This case has been reported for its rarity and its association following chicken pox, which has not been reported previously. Case report An eight-year-old male child was admitted with complaints of tightness of skin over the face and trunk for two weeks. Except for the history of chicken pox that the patient suffered from four weeks before admission, there was no other significant history of illness and other complaints. The thickening of the skin was first noticed on the face and it progressed to involve the neck, trunk, and arms over a period of ten days. On examination, the patient was alert and comfortable. He had an expressionless face with almost complete obliteration of skin folds and was unable to open his mouth completely. The skin over the face, neck, trunk, and arms was symmetrically involved and was waxy, indurated with non-pitting swelling and was non-pinchable. The lower limbs were affected to a lesser extent. There were no other skin lesions in the form of nodules, ulcers, or telangiectasia. Due to the thickening of the overlying skin, there was a minimal restriction of movements of both the shoulders without any signs of inflammation. The systemic examination was unremarkable. Investigations revealed normal haemoglobin level, blood counts, and erythrocyte sedimentation rate. The blood glucose level was normal and anti-streptolyin O titre was not raised. The tests for antinuclear antibodies, anti double stranded DNA antibodies and rheumatoid factor were negative and the serum immunoglobulin-G levels were not raised. The skin biopsy showed a normal epidermis, but the dermis was thickened with an increase in the collagenous tissue. There were slit like empty spaces between collagen bundles suggestive of oedema in the dermis. An alcian blue staining revealed mucin deposits between the collagen bundles (Figure 1). The child was observed in the ward for a period of two weeks during which the thickening over the face resolved spontaneously with reappearance of skin creases and patient being able to open his mouth completely. Discussion Scleredema adultorum is a rare condition afflicting the dermis. Contrary to what the name suggests, the entity is seen in children with 29% cases occurring in the first decade 1 . Kumar et al have reported the condition in a six weeks old infant, who happens to be the youngest patient with the scleredema adultorum 2 . The onset of the disease is preceded in most cases by an acute febrile illness including streptococcal infection (tonsillitis, pharyngitis, and pyoderma), influenza, scarlet fever, measles, and mumps 1 . Cases following tuberculous lymphadenitis and trauma have also been cited 3 , but a case following chicken pox has not been reported so far. Up to 95 percent of these cases have silent period of one to six weeks following an acute febrile illness followed by the classical symptomatology, which includes thickened skin and its attendant effects (inability to open mouth, mask-like face, inability to wrinkle forehead, restricted chest and joint movements) as the only manifestations. Occasional cases with systemic involvement in the form of dysarthria, dysphagia, pleural, pericardial and peritoneal effusions, hydroarthrosis, Wolff-Parkinson-White syndrome and trophic corneal disturbances, haemorrhagic bullae, limitation of tongue and ocular movements have also been reported 3-6 . Scleredema has been associated with a number of other illnesses. Long-standing diabetes and obesity are the most common of such conditions 1,3 . It has also been associated with monoclonal gammopathy, hyperparathyroidism, multiple myeloma, malignant insulinoma, rheumatoid arthritis, and Sjogren's syndrome. The pathogenesis of the condition remains obscure and possible hypotheses implicating immune mechanisms (an autoimmune disease secondary to sensitisation of the collagen by the products of an infectious agent), direct action of bacterial toxin and effects of adrenal steroids released in response to infection have been put forward 3,7 . The condition has to be differentiated from scleroderma, trichinosis, dermatomyositis, myxedema, progeria, papular mucinosis and oedema of cardiac or renal origin 8 . Besides clinical manifestations and laboratory tests, skin biopsy revealing dermal thickening, which is due to the accumulation of predominantly hyaluronic acid, an acid mucopolysaccharide and other glycosoaminoglycans identified using special stain as mucin threads located in the spaces among swollen collagen bundles, helps in confirming the diagnosis. Infiltration of mucopolysaccharides is also seen in conditions like lupus erythematosous, dermatomyositis, keloids, localised myxedema, papular mucinosis, myxoid cyst, alopecial mucinosa, and pseudoxanthoma elasticum. It appears that this is a non-specific response in which the fibroblasts are stimulated to elaborate mucopolysaccharides 3 . Such conditions can be easily ruled out on clinical grounds by other associated manifestations or by the specific diagnostic tests. There is no definitive therapy for scleredema. Physiotherapy may help to prevent the restrictive effects on the muscles and joints. Many forms of therapy including antibiotics, corticosteroids, thyroid hormones, pituitary extracts, estradiol, hyaluronidase, ethylene diamine tetra acetic acid, para amino benzoic acid, fibrolysin, pilocarpine and thorium-X, hot baths, radiant heat, ultraviolet radiation, fever therapy with typhoid vaccine have been tried with contradictory results 3,6 . The condition is usually self-limiting with active phase persisting for two to eight weeks followed by spontaneous and complete resolution in six months to two years. Occasional cases with no resolution even after 10 years have been cited 3 . Scleredema occurring in absence of a prodrome may remain static or progress slowly over many years, while that occurring in association with diabetes and obesity has an extensive involvement and a prolonged course 9 . Uncommonly, a rapid fatal outcome has been described 10 . Recurrences are extremely rare. The patient reported here had spontaneous resolution and had made an uneventful recovery. The occurrence of scleredema following chicken pox is important to keep in mind to avoid extensive expensive investigations to rule out other conditions mimicking scleredema. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00024f1.jpg] |
| |||||||||

{kind=link}