 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 96-97 Case Report Sprengels Deformity: Anaesthesia Management Dave S, Naik LD Department of Anaesthesiology,
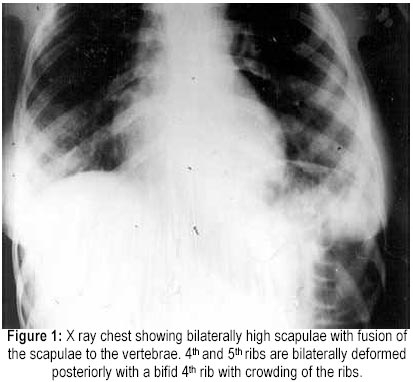
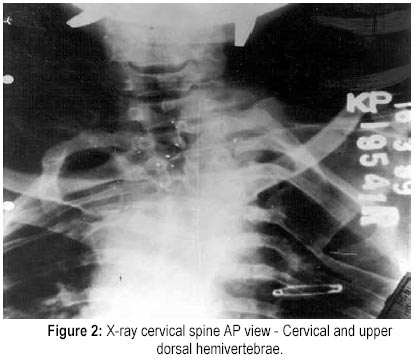
Seth G. S. Medical College and K. E. M. Hospital, Parel, Mumbai - 400 012, India. Code Number: jp00026 Abstract: A 28 years old lady presented with Sprengels deformity and hemivertebrae for Fothergills surgery. Clinically there were no anomalies of the nervous, renal or the cardiovascular systems. She had a short neck and score on modified Mallampati test was grade 2. She was successfully anaesthetised using injection Propofol as a total intravenous anaesthetic agent after adequate premedication with injection Midazolam and injection Pentazocine. Patient had an uneventful intraoperative and postoperative course. (J Postgrad Med 2000; 46:96-97) Key Words: Sprengels deformity, Hemivertebrae, Fothergills Surgery Sprengels deformity is a congenital deformity with upward displacement of scapula without rotation. It may be associated with other congenital deformities like absence or fusion of ribs, cervical ribs, the Klippel- Feil syndrome, congenital scoliosis with hemivertebrae and spina bifida in the cervical region, syringomyelia, paraplegia, situs inversus and mandibulofacial dystosis. There may be a host of other associated skeletal, renal or cardiac anomalies, making the anaesthetic management challenging. Here we describe the anaesthetic management of a case of Sprengels deformity. Case report A 28-years-old lady weighing 40 kg and measuring 140 cm in height presented with uterine prolapse for Fothergills surgery with anteroposterior repair. There was no history suggestive of any major illness in the past. She had undergone tubal ligation under general anaesthesia uneventfully four months prior to this surgery. She had a shoulder deformity since childhood. There was no history suggestive of a neurological deficit, breathlessness or limitation of the shoulder joint associated with it. On examination, her vital parameters were within normal limits. Mouth opening was adequate and score on modified Mallampati test was grade 2. She had protruding upper teeth. There was no limitation of flexion or extension at the cervical spine, but the cervical spine appeared short. Bilaterally the scapulae were elevated. There was thoracic scoliosis and the lumbar spine was not well palpable. Her respiratory system was normal and her breath holding time was 20 seconds. All routine investigations including arterial blood gases, ECG, and renal parameters were normal, except the x-ray chest, which showed bilaterally high scapulae with fusion of the scapulae to the vertebrae (Figure 1). There was also evidence of cervical and upper dorsal hemivertebrae (Figure 2). The fourth and fifth ribs were bilaterally deformed posteriorly with a bifid right fourth rib. There was crowding of upper ribs. The cardiac shadow and both the lung fields were normal. The x-ray findings were suggestive of Sprengels deformity. X-ray lumbar spine was normal. An indirect laryngoscopy revealed an overhanging epiglottis, with part of the posterior cord and arytenoids seen. Written informed consent was taken after explaining the risk of anaesthesia to the patient. Routine pre-anaesthesia precautions and procedures were followed. Difficult intubation cart was kept ready. Both the shoulders were padded to prevent any injury to the brachial plexus. Patient was sedated with injection Midazolam 1.3 mg and injection Pentazocine 24 mg. Patient was induced with injection Propofol 90 mg (mixed with injection Xylocard 10mg) intravenously. Patient was given lithotomy position taking care of her shoulder joints and spine. Paracervical block was given with 10 cc of 1% lignocaine and 20 cc of 0.25% sensorcaine. Patient was maintained on Propofol infusion. The infusion rate was titrated between 9 mg/kg/hour and 4 mg/kg/hour to maintain adequate depth of anaesthesia. Surgery proceeded smoothly with the patient maintaining adequate depth of anaesthesia. Surgery lasted for 1 hour and 5 minutes. Patient was fully awake three minutes after stopping the infusion. Total dose of propofol required throughout surgery was 370 mg. There were no untoward post-operative complications. Discussion Sprengels deformity is an asymmetry of the shoulder caused by the upward and forward displacement of the scapula. There is a broad osseous band connecting the scapula with the spinous process of the sixth cervical vertebra. The level of the scapula may be 1 to 12 cms higher than normal. The neck is fuller and shorter and the cervicoscapular line is diminished. This may pose an unexpected difficult intubation 1 . The shoulder girdle is usually defective. The trapezius is most severely affected and may be absent or weak. The rhomboids and levator scapulae are usually hypoplastic and fibrosed 1 . Examination of the musculature is imperative and nerve blocks should be avoided. Scoliosis and kyphosis due to congenital deformity of the vertebrae may be present 1 . Adequate workup of a patient with congenital spinal deformities like hemivertebrae is necessary. Particular attention should be paid to cardiac, neurological and genitourinary systems as many patients have associated anomalies. 20-30 % of the patients may have associated genitourinary tract anomalies. 10% of the patients may have congenital heart disease and 5 -10 % of the patients may have spinal dysraphism including diastomyelia, tethered chord and fibrous bands 2 . In view of the likely association of neurological anomalies in these patients, it was decided to avoid regional anaesthesia and to conduct the case on total intravenous anaesthesia supplemented with a local block. This would avoid the trauma and morbidity associated with a difficult intubation, the likelihood of which could not be ruled out in such cases. Propofol is a rapidly acting hypnotic which is used for intravenous anaesthesia. It has a brief duration of action due to redistribution and metabolism. It is not cumulative after repeated injections. Total intravenous anaesthesia with propofol is smooth, with a reduced incidence of coughing and hiccups, as compared with barbiturates and etomidate. It has fewer incidence of postoperative nausea and vomiting. Thus, propofol is a good hypnotic for use as a continuous infusion to maintain hypnosis in total intravenous anaesthesia. The dose required is 6-12 mg/kg/hour after a bolus dose 3 . Because of the rapid return of respiration and awakening, lack of postoperative side effects including vomiting, total intravenous anaesthesia using propofol with good premedication and oxygen supplementation provides excellent anaesthesia for surgeries lasting for an hour or less. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00026f2.jpg] [jp00026f1.jpg] |
| |||||||||

{kind=link}
{kind=link}