 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 98-100 Case Report Neurofibromatosis-Noonan Syndrome or LEOPARD Syndrome? A Clinical Dilemma Tullu MS, Muranjan MN, Kantharia VC, Parmar RC, Sahu DR, Bavdekar SB, (Late) Bharucha BA Genetics
Division, Department of Paediatrics, Seth G. S. Medical College & K. E. M. Hospital,
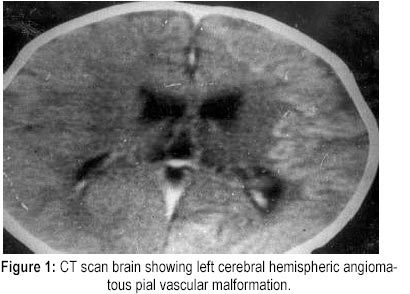
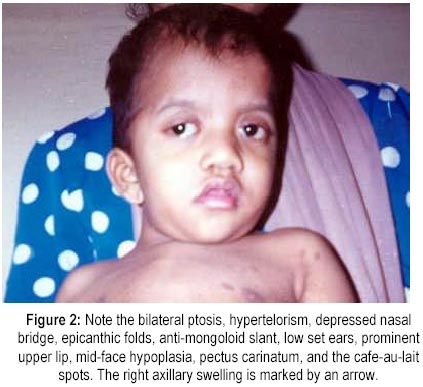
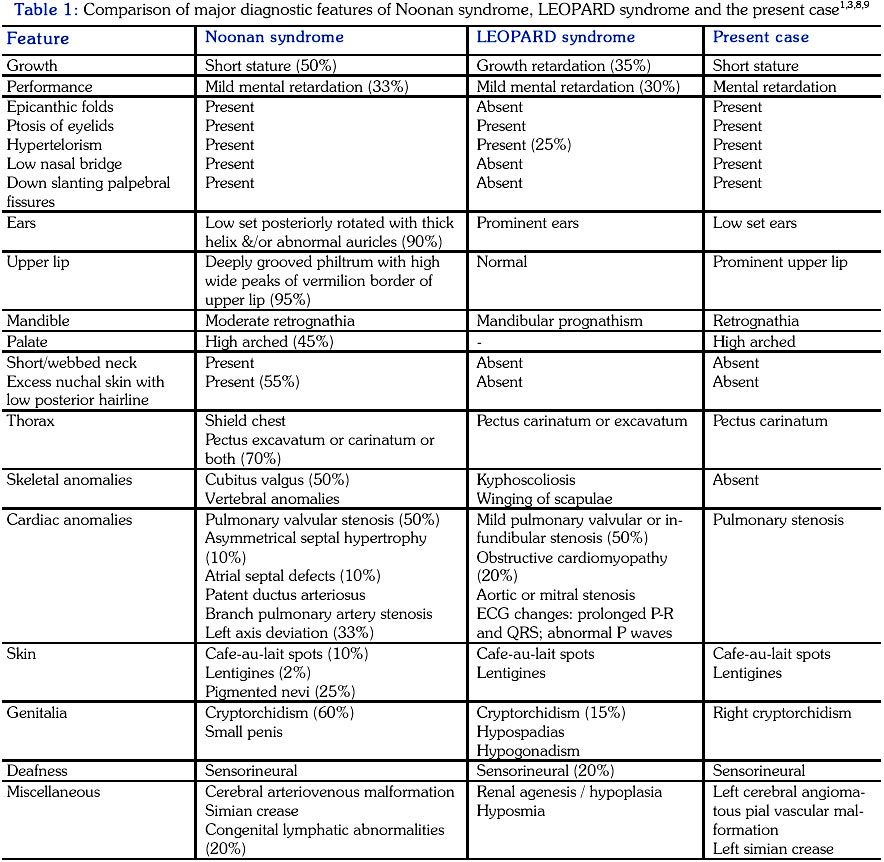
Parel, Mumbai - 400 012, India. Code Number: jp00027 Abstract: Neurofibromatosis (NF), Noonan syndrome (NS), and LEOPARD syndrome are all autosomal dominant conditions, each being a distinct clinical entity by itself. Rarely, one encounters cases with features of NF and NS and is termed as the 'Neurofibromatosis-Noonan syndrome' (NF-NS). The authors report a clinical dilemma with major clinical features of the NF-NS syndrome and LEOPARD syndrome co-existing in the same patient. Also, features of Noonan syndrome and LEOPARD syndrome are compared with the case reported. (J Postgrad Med 2000; 46:98-100) Key Words: Neurofibromatosis, Noonan syndrome, LEOPARD syndrome, Lentigines, Pulmonary stenosis, Cafe-au-lait spots Noonan syndrome (NS) is fairly common and occurs with an incidence of 1:1000 to 1:2500 live births 1 . Neurofibromatosis (NF) is also common and affects 1 in 3500 individuals 2 . A few patients with characteristics of both NF and NS have been described and are called as the Neurofibromatosis-Noonan syndrome (NF-NS) 1 . LEOPARD syndrome is a rare multisystemic disorder characterised by Lentigines, ECG abnormalities, Ocular hypertelorism, Pulmonic stenosis, Abnormalities of genitalia, Retardation of growth, and Deafness 3 . There are many features common to NF-NS and LEOPARD syndrome as seen in this interesting case. Case Report A 15 months-old-male child born of a third degree consanguineous marriage presented with global developmental delay and recurrent respiratory infections. His antenatal and birth history were normal. At the age of two months, he had refusal to feed and breathlessness and was diagnosed to have pulmonary stenosis for which a balloon valvoplasty was successfully performed. An episode of fever provoked a generalised tonic clonic convulsion at the age of eight months and was followed by right hemiparesis. A CT scan of the brain done at that time revealed left cerebral hemispheric angiomatous pial vascular malformation and mild cerebral cortical atrophy (Figure 1). The CSF examination was normal and EEG showed left hemispheric slowing with low amplitude. On examination, he had growth failure, microcephaly, and decreased ear length. Craniofacial dysmorphisms included coarse facies, depressed nasal bridge, bilateral ptosis, and low set ears. The child had right hemiparesis, pectus carinatum, right-sided cryptorchidism with poorly developed scrotum, and multiple pigmented macules along with multiple cafe-au-lait spots. A grade IV/VI systolic murmur was present in the pulmonary area with a single second heart sound. The developmental age was six months. At the age of four years additional features noticed included prominent upper lip, anti-mongoloid slant of palpebral fissures, high arched palate, retrognathia, epicanthic folds, midface hypoplasia, and left hand simian crease (Figure 2). The developmental age was one year with a developmental quotient of 39. Multiple pigmented spots of size 1 to 5 mm were noticed all over the body and cafe-au-lait spots ranging from 1 to 4 cm were also present. There was a firm swelling in the right axilla about 3 x 3 cm in size (Figure 2). Investigations including complete blood count, renal function tests, arterial blood gases, and bleeding profile were normal, as was the fundus. ECG showed right ventricular hypertrophy. Abdominal ultrasonography was normal. Colour Doppler showed severe stenosis of the pulmonary artery with a transvalvular gradient of 98 mmHg. His brainstem evoked response audiometry revealed bilateral moderate sensorineural hearing loss. The karyotype was normal. Skin biopsy of the smaller pigmented macules was suggestive of lentigines with an increase in the rete ridges in the basal layer. The parents were normal and did not have neurocutaneous lesions on Wood's lamp examination. Discussion Cases with overlapping clinical features of NS and NF have been reported (Neurofibromatosis-Noonan syndrome) 1,4-7 . The LEOPARD syndrome is comparatively rare and there are no reports of coexisting NS, though 2% of the cases with NS have lentigines 1 . The comparative features of NS, LEOPARD syndrome, and our case are presented in Table 1. As can be noted from the table, most of the diagnostic criteria for the LEOPARD syndrome except the ECG abnormalities (or cardiomyopathy) were present in our case. Though the craniofacial features in our case were characteristic of NS, webbing of neck was absent. The presence of significant cafe-au-lait spots prompted a careful search for other features of NF-1, which were absent. The child did have an axillary swelling, which could very well be a neurofibroma. Unfortunately, it could not be biopsied due to the high-risk cardiac status of the patient. Neurofibromas rarely develop before six years of age as do the other major manifestations of NF such as the Lisch nodules 2 . Our patient will need a close follow-up over the years to detect an evolving NF-1 phenotype. As a point of interest, both NF and LEOPARD syndrome have an autosomal dominant inheritance 2,3 . An apparent autosomal dominant transmission has been reported in NS as well 8 . All the three syndromes have a variable expression so that it is not mandatory for all the clinical features to be present to make a diagnosis 2,3,8 . Various theories have been proposed to explain the co-existence of NF and NS. These include- a coincidental event, new mutation, predisposition of NS to neural crest dysplasias, etc 4-7 . None of these have been substantiated beyond doubt. The gene for NF-1 is located at 17q11.2 10 and that for NS at 12q22-ter 8 . As yet there is no evidence to suggest the existence of a distinct locus for NF-NS. It is hoped that with the rapid advances in the field of molecular genetics, it will be possible to solve clinical dilemmas like the present case. Acknowledgements We thank our Dean for his permission for the publication and Dr. Deepak Parikh, Consultant Dermatologist, Bombay Hospital for performing and interpreting the skin biopsy. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00027t1.jpg] [jp00027f2.jpg] [jp00027f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}