 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
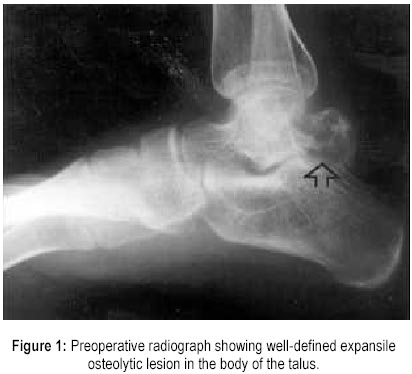
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 110-111 Case Report Giant Cell Tumour of Talar Body Bapat MR, Narlawar RS*, Pimple MK, Bhosale PB Departments
of Orthopaedics and Radiology*, Seth G. S. Medical College and K. E. M. Hospital,
Parel, Mumbai - 400 012, India. Code Number: jp00032 Abstract: Giant cell tumour (osteoclastoma) of talar bone is a rare entity and is seen more commonly in the third decade of life. We report this disease entity in a 17-year-old girl. The patient presented with painful swelling of the left ankle with an osteolytic lesion in the talus on conventional radiographs. Intralesional curettage and autologous bone grafting was performed following which patient's pain and swelling disappeared. Complete range of movement at the ankle joint was regained with minimal restriction at the subtalar joint. There is no evidence of relapse at six months follow up. (J Postgrad Med 2000; 46:110-111) Key words: Giant cell tumour, Talar bone, Intralesional curettage, Relapse. Giant cell tumour (GCT) is most commonly seen in the distal femur, the proximal tibia and the distal radius and the proximal humerus in descending order of frequency 1 . GCT is uncommon in the small bones of the hand and feet and a very few cases have been reported. GCT of talus is an uncommon finding and very rarely reported 2,3 . The classical treatment of choice is intralesional curettage. In recent times, cementing and cryotherapy is increasingly been used with encouraging results. Recurrence is very common in this locally aggressive benign neoplasm. Case report A 17-year-old girl presented with gradually increasing pain in the right ankle following a trivial trauma two months back. The symptoms had gradually increased in intensity with appearance of a swelling on the dorso-lateral aspect of the foot since fifteen days. On examination, the swelling was tender and bony hard in consistency with ill-defined margins. There were restricted movements of subtalar joint, but the ankle movements were free. The patient had an antalgic gait and the symptoms aggravated on walking on uneven ground. The radiograph of the ankle revealed an osteolytic expansile lesion in body of talus, which had ballooned, and the cortex had thinned out (Figure 1). The margins of the ankle and the subtalar joints appeared normal. The haemogram revealed a normal haemoglobin, white cell count and erythrocyte sedimentation rate. The patient was posted for intralesional curettage with bone grafting. Cementing was not contemplated, as it was feared that the subchondral placement of cement might cause early degeneration of the articular cartilage. Intraoperatively, there was no involvement of articular cartilage or evidence of pathological fracture. An intra-lesional curettage and bone grafting was performed. The bone graft was mixed with hydroxy-appatite granules. Histopathology revealed the diagnosis of giant cell tumour. A protective cast was applied for a period of three months. The patient was subsequently mobilized to full weight bearing status. A follow up of six months revealed minimal restriction of subtalar movements. The ankle movements were normal. There was no evidence of recurrence. Discussion Giant cell tumour is a benign but locally aggressive neoplasm with a tendency for local recurrence. This tumour generally occurs in skeletally mature individuals with its peak incidence in the third decade of life. The most common sites of involvement are the distal femur, the proximal tibia and the distal radius, but the sacrum, the distal tibia, the proximal humerus, the proximal femur, and the proximal fibula are not infrequent sites. Rarely, the tumour is found in other sites such as the bones of the hands and, the feet, the vertebral bodies above the sacrum, and the ribs 2. Giant cell tumour of the small bones of the hand and foot seem to occur in a slightly younger age group and demonstrate a higher incidence of multicentricity than those in other locations 3 . Clinically GCT of the talus presents as ankle sprain or sinus tarsi syndrome with or without history of trivial trauma. In long tubular bones radiologically the differential diagnosis include Aneurysmal bone cyst, nonossifying fibroma and chondroblastoma. When giant cell tumour occurs in long bones, conventional radiographs demonstrate a lytic lesion centred in the epiphysis but involving the metaphysis and extending, at least in part, to the adjacent articular cortex. The tumour usually bulges beyond the confines of the cortex, which has undergone varying degrees of resorption. Apart from a thin shell of subperiosteal new bone outlining the outer surface of the tumour, no periosteal reactions are appreciated unless a fracture is present. However, the radiographic features of giant cell tumour at sites other than the long bones are non-specific and are not unlike other osteolytic processes 4 . The standard treatment
of giant cell tumour of bone traditionally has been intralesional excision of
curettage and autograft reconstruction by packing the cavity of the excised tumour
with morselised iliac cortical and cancellous bone. Intralesional excision however
leaves microscopic disease in the bone regardless of how carefully or thoroughly
performed. The reported incidence of local relapse with this technique is high
as 40-60% 4 . There has been a great deal of effort expended on attempt
to extend the curettage or excision by chemical or physical means. Chemicals such
as phenol or cytotoxic agents like chlorpactin have been applied to the tumour
bed to decrease the relapse with varying results 5 . Cryosurgery using
liquid nitrogen to extend the curettage has a high incidence of local wound and
bone complications. Packing the tumour bed with methylmethacrylate has shown to
decrease the relapse rate by generating local hyperthermia, which induces necrosis
of any remaining neoplastic tissue. In addition, the polymerisation of methylmethacrylate
may produce a local chemical cytotoxic effect. However, it is feared that the
subchondral placement of cement may induce degeneration of the articular cartilage.
There is a limited experience with the CO2 laser for cauterising the
tumour bed. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00032f1.jpg] |
| |||||||||

{kind=link}