 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
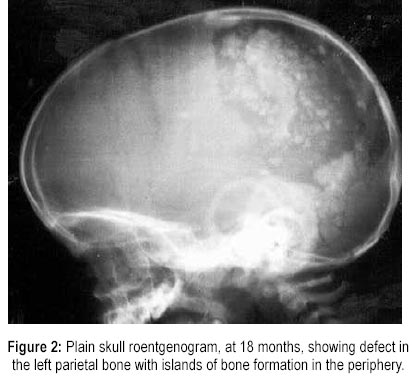
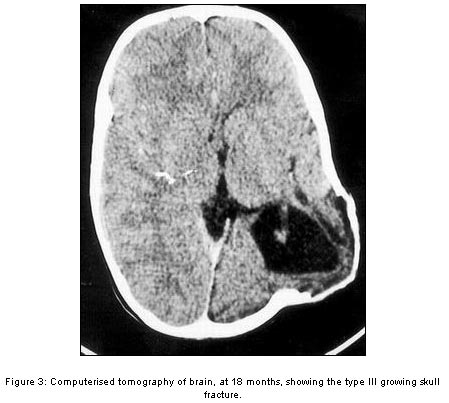
Journal of Postgraduate Medicine, Vol. 46, No. 2, April-June, 2000, pp. 130-131 Images in Radiology: Type III Growing Skull Fracture Parmar RC, Bavdekar SB The Department of Paediatrics, Seth G. S. Medical College and
K. E. M. Hospital, Parel, Mumbai - 400 012. Code Number: jp00037 A six months old male infant presented with convulsion following an episode of fall. The clinical examination did not reveal any abnormality. Plain skull roentgenogram revealed a non-depressed left parietal fracture (Figure 1). Computerised tomographic (CT) scan of brain was normal. The patient was treated conservatively and was advised to follow up. Subsequently, the patient was seen again at the age of 18 months with a gradually enlarging swelling over the scalp and right-sided hemiparesis. Repeat plain skull roentgenogram revealed a large skull defect in the left parietal bone with smooth margins and islands of bone formation in the periphery (Figure 2). The CT scan of the brain revealed presence of a skull defect in the left parietal region and a hypodense cystic lesion herniating through the defect. The left superolateral parietal lobe showed loss of substance with porencephalic dilatation, which reached laterally to the superolateral cortex and medially towards the body of the lateral ventricle (Figure 3). Based on this a diagnosis of type III growing skull fracture (GSF) was made. The patient underwent excision of the cyst with dural repair, but presented with a recurrence of the leptomeningeal cyst at 21/2 years. The patient was then advised cranioplasty with excision of the cyst. Discussion Most skull fractures in childhood heal rapidly without any complication. However, in a miniscule minority, a fracture may remain unhealed and enlarge to form a growing skull fracture. In 1816, John Hopkins described an infant with GSF following head trauma. Since then, cases of GSF continue to appear in the literature under varied terminologies like leptomeningeal cyst, traumatic meningocoele, cerebrocranial erosion, cephalohydrocoele, meningocoele spuria, etc. GSF is a rare complication affecting 1.2 to 1.6% of severe head injury with a vast majority of cases occurring in children under three years of age 1-3 . But, cases presenting as early as in the perinatal period and as late as six decades after the initial insult have been described 4,5 . The majority of cases occur following falls, vehicular accidents, and child abuse. Cases following difficult vacuum extraction and corrective surgery for craniosynostosis have also been described 6,7 . Most GSFs are located in the calvarium; other sites include basiocciput and orbital roof. Exact pathophysiology of the GSF still remains debatable. The factors incriminated for the GSFs include head injury with large fracture, presence of a dural tear, parenchymal injury beneath the skull and dural defect, and injury during the period of maximum brain growth. A combination of these factors alters the normal distribution of intracranial tension and the fracture behaves like a neosuture with abnormal growth of the skull at the fracture site. Following the initial head trauma, patients with GSF usually present with gradually enlarging subgaleal mass, seizures, headache, or focal neurological deficit. Diagnosis is based on clinical and radiological evaluation. Serial plain skull roentgenograms show evolution of the initial diastatic fracture into a larger defect. Albeit, plain roentenography is sufficient to diagnose the condition, CT scan of brain remains the investigation of choice to define the exact pathology. Based on the CT appearance, GSFs are subdivided into three types. The type I GSF refers to GSF with a leptomeningeal cyst, which may be seen herniating through the skull defect into the subgaleal space. In type II lesion damaged or gliotic brain and in type III a porencephalic cyst can be seen. An increasing order of the defect is associated with an increasing severity of the neurological deficit. While CT scan can pickup an already established lesion, magnetic resonance imaging has an advantage of detecting dural tear immediately following the head trauma and a timely correction can be helpful in the prevention of growth of the fracture. A few authorities use cranial Doppler studies for an early diagnosis 8 . The treatment is surgical and consists of reduction of the herniated cerebral tissue and repair of the dural laceration or cranioplasty. A shunt surgery may be performed to decompress the cyst and treat localised dilatation of the ventricles. Prompt recognition and early diagnosis are essential to prevent the development of neurological complications. Hence, it is essential to follow up cases of head trauma radiologically and clinically until healing occurs. References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00037f3.jpg] [jp00037f2.jpg] |
| |||||||||

{kind=link}
{kind=link}