 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 3, July-September, 2000, pp. 215-216 Images in Pathology Functioning Oxyphil Adenoma of Parathyroid Dewanda NK, Chumber S, Tandon N*, Karak AK** Departments of Surgical Disciplines, Endocrinology*and Pathology**, All India
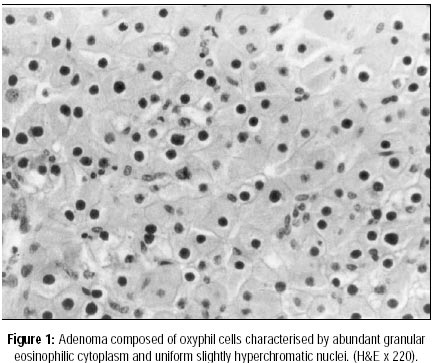
Institute of Medical Sciences, New Delhi, India. Code Number: jp00075 A 45-year-old lady presented with multiple joint pain for the last 6 years. She was initially treated for rheumatoid arthritis; as she did not respond, she was further evaluated and a diagnosis of hyperparathyroidism was made. At presentation, she had mild pedal oedema and tenderness over the twelfth thoracic and first lumbar vertebra. Laboratory findings revealed serum calcium values of 10.04, 10.74 and 10.84 mg/dL on three occasions, (corrected for serum albumin 4.2 mg/dL). The 24-hour urinary calcium was 903 mg/24 hr and phosphate was 120 mg/24 hr. The serum parathyroid hormone level was 1291.0 pg/ml (normal limits 10-54 pg/ml). The serum alkaline phosphatase was 582 IU/dL. The x-rays of the skull showed a salt and pepper appearance, those of hands showed subperiosteal bone resorption and erosions of the phalanges and the metacarpals, the x-ray of the pelvis, skull and hands showed decreased bone density. An ultrasound of the neck showed a hypodense lesion in the left lower part of the neck in the parathyroid region measuring 8 x 16 mm. A Technetium-thallium subtraction scan showed increased activity in the region of left upper side of the neck. At surgery a 3 x 2 x 1 cm and 3.17 gm mass was excised from the left lower parathyroid, which was reported as an adenoma on frozen section. On histopathological examination, the left lower parathyroid gland revealed a well-encapsulated oxyphil cell adenoma (Figure 1). There was focal thin rim of normal parathyroid tissue in the edge. The oxyphil cells were large, with abundant eosinophilic granular cytoplasm and small regular nuclei and sharp borders. The other excised parathyroid was normal. Postoperatively, the patient developed symptomatic hypocalcaemia with serum calcium falling to 7.3 mg/dL which responded to calcium supplement and vitamin D3. During the follow-up period she has done well.
Discussion Adenomas of the parathyroid glands are the most frequent cause of primary hyperparathyroidism, majority of which are chief cell tumours.1 Oxyphil adenomas of the parathyroid are uncommon and have been considered non-functioning in past.2,3 However, there is evidence to suggest that oxyphil cell adenoma can be functioning and capable of producing parathyroid hormone.2-4 In Multiple Endocrine Neoplasia (MEN) syndromes types I and II, the predominant parathyroid lesion is an asymmetric nodular hyperplasia of the chief cell and uncommonly an adenoma. Oxyphil adenomas (oncocytomas) are rare benign tumours representing about 0.01% of neoplasms of the head and neck.5 Warren and Morgan,6 in 1935, were first to report a functional pure oxyphil adenoma of the parathyroid. Since then a number of authors have reported functioning oxyphil adenoma of the parathyroid.1-4,7 Poole et al,4 on reviewing the literature in 1982, found about 50 cases reported of functional oxyphil adenoma. The diagnostic criteria for functioning oxyphil adenoma include (a) at least 90% of the adenoma be composed of oxyphil cells, (b) a biopsy or excision of a second histologically normal parathyroid gland excluding the diagnostic possibility of hyperplasia and (c) postoperative alleviation of hypercalcaemia.7 This case fulfils all the three criteria. On localisation studies, an ultra-sound as well as a Thallium-Technetium subtraction scan, an adenoma at best can be localised as being present either as on left side or right side. It is difficult to be sure that an identified adenoma is in an upper or a lower parathyroid. Hence a slight variance from the surgical findings may be seen. Arnold et al,2 in 1974, reported elevated levels of parathyroid hormone in the jugular vein draining a pure oxyphil adenoma and demonstrated prominent Golgi apparatus in these cells. McGregor et al3 demonstrated that isolated oxyphil adenomatous tissue could synthesise proparathormone and parathormone. Secretory granules in these cells have been demonstrated and the cytoplasm has been reported to be extremely rich in mitochondria.2-4 Poole et al4 on staining of pure oxyphil adenoma by immunoperoxidase technique found the parathyroid hormone to be dispersed throughout the cytoplasm, with the area of greatest concentration lying just beneath the cell membranes, where the secretory granules have been seen by electron microscopy.
References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00075f1.jpg] |
| |||||||||

{kind=link}