 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 4, October-December, 2000, pp. 265-267 Modified Mesh Rectopexy: A Study Bakshi G, Ranka S, Agrawal S, Shetty SV Surgery Department, Seth G. S. Medical College and Dr R. N. Cooper Hospital,
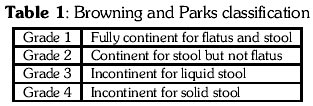
Vile Parle, Mumbai. Code Number: jp00089 Abstract: AIM: To evaluate the efficacy of modified mesh rectopexy for complete rectal prolapse. SUBJECT AND METHODS: In a prospective study between 1989-1998, 47 patients (25 males and 22 females) underwent modified mesh rectopexy using a "Cross-shaped" knitted monofilament polypropylene. They were followed up for a period of four years postoperatively. RESULTS: Anatomical repair was achieved in all patients. Preoperative constipation, a complaint in 22 patients, was relieved in 13 patients and need for laxatives decreased in another four. There were no new cases of constipation. Sexual functions were not hampered irrespective of gender. The complications included prolonged ileus (4 patients), faecal impaction (1), partial mucosal prolapse (2) and post-operative obstruction (2). There was no recurrence. CONCLUSION: This technique aligns the rectum, avoids excessive mobilisation and division of lateral ligaments thus preventing constipation and preserving potency. We recommend this technique for patients with complete rectal prolapse with up to grade 1, 2 and 3 incontinence based on Browning and Parks classification. (J Postgrad Med 2000; 46:265-267) Key Words: Prolapse, Polypropylene, Incontinence, Constipation. Rectal prolapse is a distressing condition especially when associated with faecal incontinence and constipation. It usually occurs in children or elderly. Presently laparoscopic approach is favoured as it has better results especially in terms of less post-operative pain, shorter hospital stay and lower cost.1,2. This facility is not available universally, nor the expertise needed for it. Abdominal approach is still favoured by the conventional colo-rectal surgeon who is well versed with the technique and its outcome.3 A 10-year experience with modified mesh rectopexy (MMR) has been reviewed.
Subjects and Methods This is a prospective, single centre, open study carried out in 47 consecutive patients with reducible complete rectal prolapse, from 1989 to 1998, to evaluate the efficacy of Modified Mesh Rectopexy. Permission of ethics committee of the hospital was taken. Complete rectal prolapse was defined as per Goligher's criteria.4 Of the 47 patients 25 were males and 22 females. Patients with grade 4 of Browning and Parks classification5 of incontinence (Table 1) and ASA grade IV and V were excluded. There was no history suggestive of underlying neuro-muscular abnormality in any patient and no history of obstetric trauma in females. Sexual function in males was assessed in terms of maintenance of erection, flaccidity, premature ejaculation and retrograde ejaculation postoperatively. Conception was assessed in females as six females were in reproductive age group in the study. Sexual function was not assessed in the rest 16 female patients. Four patients had a history of surgical intervention in past. Thiersch stitch was performed in three patients and in one patient abdominal approach was performed, details of which were unavailable. Constipation was the commonest complaint (22 patients) followed by incontinence (four patients) other than rectal prolapse itself. All patients underwent MMR trans-abdominally.
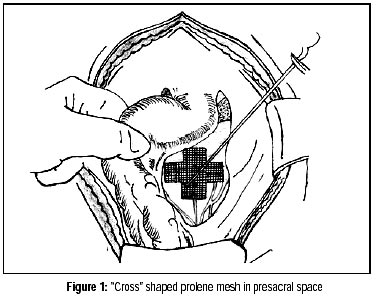
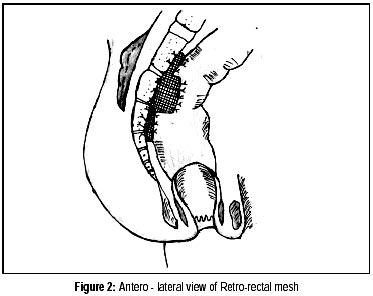
Preoperative preparation: Patient is given soft diet two days prior to the surgery. Metronidazole is given for bowel preparation, simple enema on night before and day of surgery. At induction, intravenous antibiotic i.e. third generation cephalosporin with aminoglycoside and metronidazole were administered and continued for 48 hours later. Technique: The patient was placed in moderate Trendenlenberg position after catheterisation. The rectum was mobilised by dividing the peritoneal reflection on either side. Pre-sacral space was entered and rectum mobilised up to the coccyx. Presacral nerves and ureters were routinely identified and safeguarded. Lateral ligaments were preserved in all cases. A monofilament knitted polypropylene mesh of size 15x15 cms cut in the shape of the cross as per individual requirement was placed in presacral space (Figure 1). The centre of the mesh was anchored the rectum to the sacral promontory with few 2-0 prolene sutures. The side arms of the cross encircles three-fourth the circumference of the rectum and upper and lower arms are sutured to posterior one-fourth of the rectum with the sacrum (Figure 2). Haemostasis was achieved and suction drains were kept on either side of rectum, which were removed after 48-72 hours. Mesh was extraperitonilised by resuturing back the divided peritoneal folds. Abdominal cavity was not drained. Laxatives were given routinely to all patients for a period of 3-4 weeks postoperatively. No colonic resection was performed. Pre and postoperative courses of patients were determined with particular interest in terms of constipation, continence, sexual function and recurrence determined. Follow up was obtained in terms of physical examination and symptoms on OPD basis for a mean period of four years.
Results The age range was between 21 to 77 years (mean 33 years). Only nine patients were more than 60 year of age. The procedure initially took a longer time with experience it could be completed within 90 minutes. Anatomical control of prolapse was obtained in all patients. Overall results are depicted in Table 2.There was no mortality. Four patients had prolonged ileus. Two patients presented with adhesion-obstruction within six months of surgery, and were explored. In these patients the omentum and the small bowel were adherent to the peritoneal suture line which had given away in pararectal region. These sutures were taken to extraperitonealise the mesh. One patient developed faecal impaction which was removed manually. He was also given a stool softener for a few days later. Excision of prolapsed mucosa was undertaken in the two patients under local anaesthesia.
No patient developed a leak or intra-abdominal sepsis indicative of mesh infection or rejection. Partial mucosal prolapse was encountered in two patients on straining postoperatively. Incontinence was present in three of four patients, who gave history of incontinence preoperatively. There were no new cases of incontinence. Postoperatively constipation markedly decreased in 13 patient and need for laxatives went down in another four, in the group of 22 patients who presented with constipation. Sexual function was preserved in all. There was no evidence of premature or retrograde ejaculation and patients were able to maintain erection with out any flaccidity. Six female patients in reproductive group conceived within four years after the operation. Seven patients lost to follow up; in the remaining there was no recurrent rectal prolapse.
Discussion In this study most of the patients were below the age of 60 years, in contrast to other series.6,7 Complete rectal prolapse is thought to be due to circumferrential intussesception of the upper rectum and the recto sigmoid8 or a sliding hernia according.9,10 Placing a rectangular mesh requires extensive infero-lateral dissection and division of lateral ligaments. The cross shape of the mesh, as per the space available in para and retrorectal region corrects the defect anatomically by anchoring the rectum to the sacral promontory thus elevating, straightening and refastening it. It avoids sigmoid resection as in Frykman repair,11 division of lateral ligaments and extensive dissection infero-laterally as in Ripstein repair12 and Ivalon sponge rectopexy. 13 This prevents constipation14 and sexual dysfunction in males.15 In this study incontinence persisted in three patient of four postoperatively. They were young; with a long-standing prolapse with damage to the sphincters probably.6 Even if there was some colonic dismotility preoperatively,16 constipation improved significantly in 13 of 22 patients who were constipated preoperatively. Constipation did not develop in the rest 25 patients due to preservation of lateral ligaments, division of which may interfere with colonic motility and the anchorage provided by lower limb of the cross, thus preventing an acute angulation of the rectum.14 There was no recurrence upto a follow up of four years. We did not include the partial mucosal prolapse under recurrence as reported by Boccasanta et al.17 Patients with chronic prolapse have excoriation of perianal skin, proctitis and are more liable to infection due to transmigration of microorganisms especially anaerobic and gram negative ones. Mesh, a foreign body is prone to this infection. Hence, pre-operative and post-operative antibiotics coverage is required. In conclusion, MMR is a safe and effective technique as it does not involve division of lateral ligaments, sigmoid resection and suture lines. Also need of sophisticated instruments and expertise of laparoscopy are avoided. The only drawback is the learning curve which once mastered can be performed as an effective alternative to the standard mesh rectopexy with comparable results. This procedure will add another shot to the colo-rectal surgeons armamentarium to deal with this condition. It gives results better then to other studies who have reported a recurrence of 3-8 %.17,18 It restores the prolapse to its normal position preventing neurological damage and obliterating the deep pouch. It however does not repair the lax levators which is not always necessary and also do not strengthen the patulous anal orifice. We recommend plastic repair of these cases along with MMR.
References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00089t2.jpg] [jp00089f2.jpg] [jp00089t1.jpg] [jp00089f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}