 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 4, October-December, 2000, pp. 286-287 Images in Medicine Hashimoto's Thyroiditis with Orbitopathy and DermopathySingh SK, Singh KK, Sahay RK Department of Endocrinology and Metabolism, Institute of Medical Sciences,
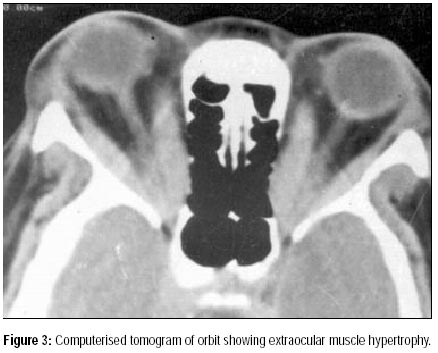
Banaras Hindu University, Varanasi - 221 005, India. Code Number: jp00095 A fifty-year female patient presented with weight gain and facial puffiness for one and half years. She was reported to have constipation, change in voice and cold intolerance since the onset of her illness. One year later she had noticed periorbital oedema and prominence of eyeballs. She had developed diminished visual acuity and occasional diplopia for one month. She was menopausal for two years. Clinical examination revealed a pulse of 80/min regular, blood pressure of 130/90 mmHg, coarse skin and normal hair. Her height was 157 cm and weight was 68 kg. Systemic examination was unremarkable. Thyroid gland was not enlarged (confirmed by ultrasonography). She had coarse velvet patch of skin over her shins (Figure 1). Eye examination showed bilateral proptosis measuring 23 mm with conjunctival injection and lagophthalmos. Lateral eyeball movement was restricted and convergence was markedly affected (Figure 2). Her visual acuity was 6/60 in both eyes. Fundus examination was normal. Intraocular tension was 40 mmHg in right eye and 42 mmHg in left eye in upward gaze only. Pupillary reaction to light was normal. She had motor power of grade 5/5 distally and 4/5 proximally. Delayed relaxation of ankle jerk was observed. Laboratory investigation included haemoglobin of 10.4 g/dl, hypochromic microcytic anaemia in general blood picture with normal WBC counts. Thyroid hormone profile by radioimmunoassay (using commercial kit supplied by BARC Mumbai) was done on two occasions and values were: T3 1.45 and 1.49 nmol/l (normal 1.1-2.9 nmol/l) T4 50.7 and 17.9 (g/dl (normal 64-154 nmol/l) and TSH 38.8 and 45mU/l (normal 0.5-3.5 mU/l). CT scan of orbit revealed marked extraocular muscle thickening (Figure 3) and anti-TPO antibody was 254 IU/ml (Ranbaxy Specialty Ltd, Mumbai, normal <50 IU/ml). Diagnosis of infiltrative orbitopathy with dermopathy with hypothyroidism was established and she was given thyroxine 150 mg with prednisolone 60-mg in divided doses and acetazolamide 250 mg twice daily. After 4 weeks of treatment her vision improved to 6/18 and lagophthalmos was absent. Steroid was tapered in 4 weeks while she continued with thyroxine replacement (150 mg/day). Discussion Autoimmune thyroid disease encompasses a spectrum of thyroid disorders with Graves' disease at one end and Hashimoto's thyroiditis at the other end. Sometimes changes of Graves' disease can supervene in the presence of histological changes of Hashimoto's disease.1 In such situation occurrence of infiltrative orbitopathy is not unusual.2 Infiltrative orbitopathy may occur in 50% of patients with Graves' disease.3 Dermopathy is late manifestation of Graves' disease and 99% patients with this feature also develop orbitopathy.4 The prevalence of orbitopathy is only 2% in patients with Hashimoto's thyroiditis.5 Patients with subacute thyroiditis and high titre of anti-microsomal antibodies have also been reported to develop ophthalmopathy similar to Graves' disease.6 Only one case report of Hashimoto's thyroiditis with ophthalmopathy and dermopathy could be found in the review of literature.7 The pathogenesis of the orbitopathy and dermopathy is not well understood. Under the influence of cytokines produced by lymphocytes, the fibroblasts secrete hydrophilic glycosamino-glycans. Accumulation of this compound impairs the function of the muscular tissue in the orbit and eventually fibrosis sets in. Such changes are also responsible for the characteristic lesions of dermopathy or pretibial myxoedema seen on the shins. Expression of TSH-receptor mRNA by retro-orbital tissue and fibroblast in the dermis has been observed and the antibodies against TSH receptor might cross react with these tissues and trigger the above cascade of events.3,8 Presence of orbitopathy and dermopathy in Hashimoto's thyroiditis can be explained on the basis of sharing of antigens of thyroid (TPO and Tg) with orbital and dermal fibroblasts and cross specificity of antibodies with these antigens. It is similar to TSH-R antigen and antibodies in Graves' disease and triggering of the events described above. Alternatively a second speculation can also be put forward. It has been reported that thyrotropin receptor antibodies (TRAB) are also expressed in Hashimoto's thyroiditis.9 However, hyperthyroidism does not occur as the cytotoxic antibodies are produced in abundance and they overcome the stimulatory effect of thyrotropin receptor antibody and cause thyroid destruction. The effect of the thyrotropin receptor antibodies on orbital and dermal tissue remains uninhibited, resulting in development of orbitopathy and dermopathy. Cronin et al7 reported a similar case of Hashimoto's thyroiditis with ophthalmopathy and pretibial myxoedema and they have also proposed that the TSH receptor antibody of Graves' disease which was raised in their case was ineffective in producing hyperthyroidism because of thyroid destruction due to Hashimoto's disease. In the present case, TSH receptor antibody activity could not be evaluated. In conclusion this case report emphasises the fact that Hashimoto's thyroiditis is at one end of spectrum of autoimmune thyroid diseases with Graves' disease being on the other end. The thyroid function varies from low to high respectively in these two forms having orbitopathy and dermopathy in common. However more observation may substantiate this supposition.
References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00095f2.jpg] [jp00095f3.jpg] [jp00095f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}