 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 46, No. 4, October-December, 2000, pp. 288-290 Images in Pathology Pseudomyxoma Peritonei Masquerading as Abdominal HydatidosisNarayana Swamy YV, Kini U*, Amirtham U*, Lahoti NK Department of Surgery & Pathology*, St.
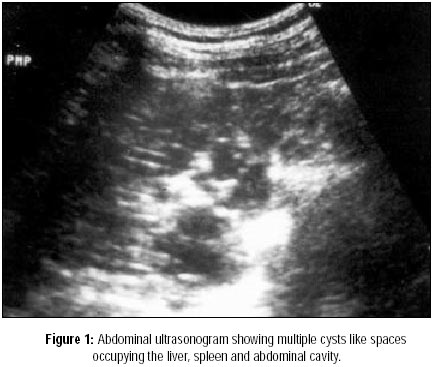
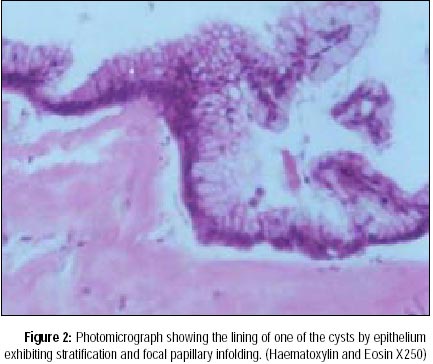
John's Medical College & Hospital, Bangalore - 560 034, India. Code Number: jp00096 A 50-year-old male presented with gradually increasing abdominal distension and right inguinoscrotal swelling of two years' duration. On clinical examination, the distended abdomen was soft, nontender, with presence of shifting dullness. A 10 x 8 cm nodular mass was felt in the right paraumbilical region with minimal intrinsic mobility. The right inguinoscrotal swelling measuring 12 x 6 cm was firm to hard and was irreducible. The right testis and cord could not be palpated separately. Abdominoscrotal ultrasonogram showed multiple echogeneic areas occupying the abdominal cavity as well as lesions in the liver and spleen suggestive of intraperitoneal hydatid disease with extension to the right scrotum (Figure 1). This was further ratified by the computerised tomographic (CT) scan of the abdomen and the pelvis. A fine needle aspiration cytology of the inguinoscrotal mass showed material resembling fragments of laminated eosinophilic material with scattered multinucleated giant cells and chronic inflammatory cells. No definite scolices were identified. As these appearances were akin to the ectocyst, a provisional diagnosis of ruptured hydatid cyst with peritoneal hydatidosis was suggested. At laparotomy an omental mass measuring 20 x 16 cms with multiple mucinous lesions were seen extending into the right scrotum through the inguinal canal. Similar lesions were identified in spleen, liver, pelvis and entire peritoneal cavity. A frozen section of the omental mass was diagnosed as mucinous neoplasm of borderline malignancy. Debulking of the omental mass and mucinous contents in the scrotum was performed with peritoneal toilet using 5% dextrose solution. Postoperative recovery was uneventful. The histopathology of the resected omental mass showed multiple cysts containing mucin and filled at foci by mucin producing tall columnar epithelium exhibiting focal stratification. A final diagnosis of Pseudomyxoma peritonei (PMP) was made and treated with cisplatin and cyclophosphamide. The patient was discharged with an advice to come for regular followup and chemotherapy. Two months later, the patient presented with features of acute intestinal obstruction necessitating an emergency laparotomy. The small bowel was dilated up to ileocaecal junction with the mass involving the caecum, appendix and ileocaecal junction. The appendix could not be easily identified as the junction was well covered by jellylike material. On careful examination, the appendix measured 7 x 4 cm and its wall was prominently thickened. Its lumen was markedly dilated and filled with mucin. The ileum was unremarkable. There was a right inguinal hernia containing myxomatous tissue densely adherent to the testis and spermatic cord. There was a reduction of about 40% of the tumour bulk as compared to the previous laparotomy. The ileocaecal mass was resected and an ileotransverse anastomosis performed along with right orchidectomy and herniorrhaphy. At histology, the appendicular mucosa exhibited some stratification, tufting, loss of polarity and hyperchromasia and an intact basement membrane (Figure 2) without evidence of tissue invasion. A histopathological diagnosis of PMP arising from borderline neoplasm of the appendix was made. The postoperative period was uneventful. The patient received three cycles of intravenous chemotherapy with cisplatin and cyclophosphamide at three weekly intervals. During the 11 months of followup he has shown no signs of recurrence.
Discussion PMP has been a subject of confusion and varied interpretation for most oncologists and many pathologists. A clear understanding of its natural history has been hampered by the fact that tumours of various sites included under the heading of PMP have significantly different biologic behaviour leading to dilemma in diagnosis and management.1 PMP is referred to as an extensive mucinous accumulation within the peritoneal cavity associated with a malignant cystic neoplasm arising commonly from the appendix or ovary; other sites include pancreas, bile duct, colon, gall bladder and urachus. Most often the patient presents with progressively increasing abdominal distension. Males commonly present with inguinal hernia while females present with an ovarian mass.2 Many cases are incidentally detected at laparotomy done for an acute abdomen such as acute appendicitis. The CT findings in PMP could be pathognomonic, characterised by selective sparing of small bowel and its mesentry separated by large volume of mucinous tumour1 and is useful in assessing the completion of cytoreduction following surgery. These studies could also be facilitated by sonographic imaging.3 A whole body scan using technetium99m MDP could also be used to accurately delineate the primary neoplasm and the region of neoplastic involvement within the peritoneal cavity.4 But, a preliminary diagnosis by either cytology and fine needle aspiration may not always be helpful as the thick mucin aspirated with poor cellularity5 could mimic the laminated membrane of the hydatid cyst as in this case and could be easily misinterpreted as ectocyst of hydatid cyst. Characteristic distribution of mucin deposits in the peritoneal cavity follow the principle of redistribution phenomenon6 based on intraperitoneal fluid dynamics favouring deposits at all sites of fluid reabsorption. They are clinically seen along the greater omentum, under surface of diaphragm, right subhepatic space, paracolic gutters, ligaments of Treitz, ileocaecal junction and pelvis. The phenomenon is assisted by the lack of adherence molecules on tumour cells, nomadic pattern of cell migration within the peritoneal space, gravity and peristaltic activity of small bowel loops. Intestinal loops are usually not involved by the process due to constant peristaltic movement but patient succumbs to it when the peritoneal surfaces are abraded as a result of a surgical procedure. The latter along with the nomadic pattern of migration of neoplastic cells within the peritoneal space and continuing proliferation of the neoplastic cells results in frequent recurrences. An aggressive initial surgical therapy is accepted as the treatment of choice for PMP.7 This includes complete debulking of gelatinous masses present within the abdominal cavity, resection of greater omentum and right hemicolectomy as the tumour often extensively involves the ileocaecal junction and right colon. Resection enblock of lymph nodes along the ileocolic artery may give prognostic information regarding lymph node metastases. Patients who present with inguinal hernia need excision of the hernial sac, herniorrhaphy, debridement of the testicle and its placement back into the scrotum. The role of adjuvant therapy in PMP has been extensively studied with the use of intraperitoneal radiotherapy with P32 and Au198 and chemotherapy seem to confer a disease free survival benefit without increased rates of complications.8 Several chemotherapeutic agents like 5-fluorouracil and MitomycinC have been tried both intravenously and intraperitoneally with variable results. An argon beam coagulator has also been used to ablate multiple peritoneal and omental implants with success.9 However, in a study of 23 cases of PMP, Wertheim et al10 concluded that surgery is the only effective therapy for this disease and that the adjuvant therapy is of doubtful benefit. One third of all patients show recurrence of disease, requiring repeated debulking surgeries. Patients with intestinal adhesions or those requiring bowel resections have a significantly high risk of intestinal fistula formation. Most of the deaths reported to have been due to intestinal obstruction.
References
This article is also available in full-text from http://www.jpgmonline.com/ Copyright 2000 - Journal of Postgradate Medicine The following images related to this document are available:Photo images[jp00096f2.jpg] [jp00096f1.jpg] |
| |||||||||

{kind=link}
{kind=link}