 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
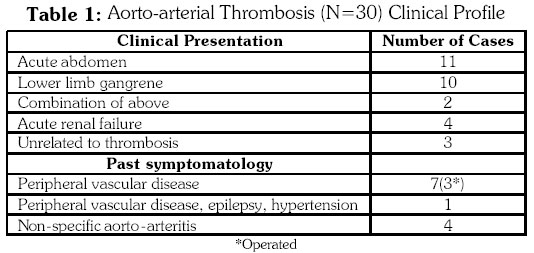
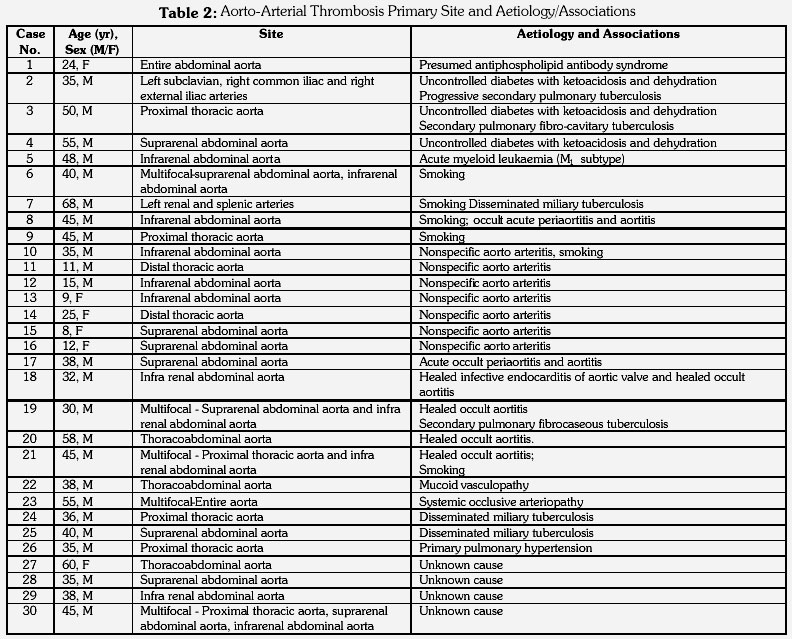
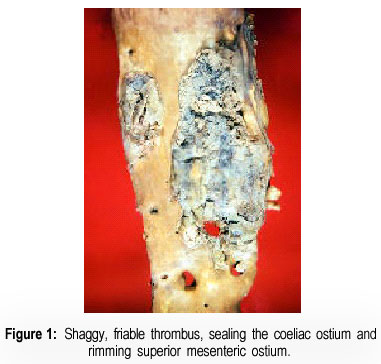
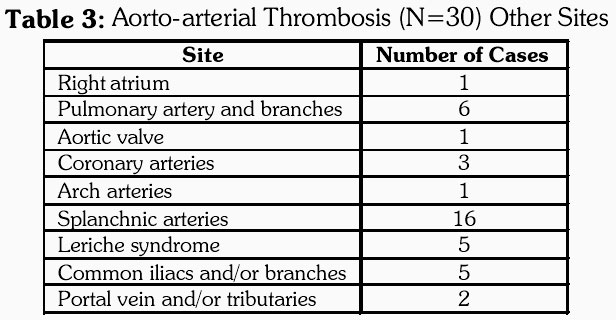
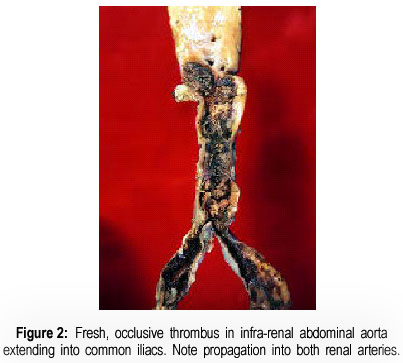
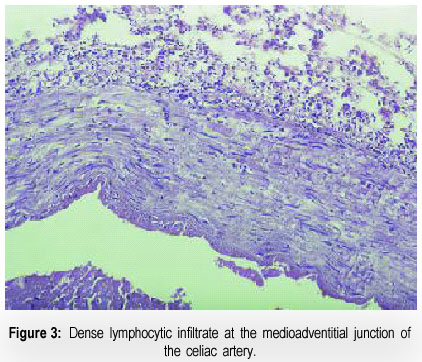
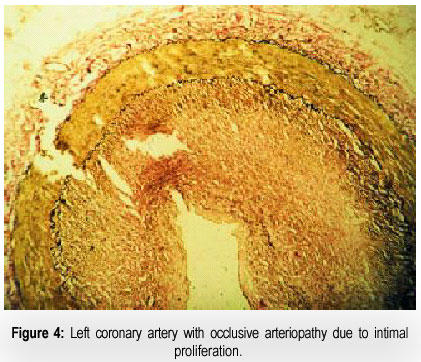
Journal of Postgraduate Medicine, Vol. 47, Issue 1, 2001 pp. 8-14 Non-Atherosclerotic Aorto-Arterial Thrombosis: A Study of 30 Cases at Autopsy Vaideeswar P, Deshpande JR Department of Pathology (Cardiovascular Division), Seth G. S. Medical College and K. E. M. Hospital, Parel, Mumbai - 400 012, India. Code Number: jp01002 Abstract BACKGROUND: Aorto-arterial thrombosis is very often associated with atherosclerotic and/or aneurysmal changes. Thrombosis, unrelated to these changes is infrequent. AIMS: To evaluate the clinical presentation and aetiopathogenesis of aorto-arterial thrombosis, unrelated to atherosclerosis and aneurysms. MATERIALS AND METHODS: A retrospective study of 30 autopsied cases of non-atherosclerotic and non-aneurysmal aorto-arterial thrombosis collected over a period of 14 years was carried out. RESULTS: There were 23 males and seven females and majority presented in the third to fourth decades of life with clinical features of acute abdomen or lower limb gangrene. Abdominal aorta as the site of thrombosis was observed in 46.5% cases. The causes were attributed to hypercoagulable states and changes in the aortic wall. No aetiology could be identified in 5 patients (16.6%). Associated tuberculosis was seen in six cases. CONCLUSIONS: Non-atherosclerotic aortic thrombosis is a heterogeneous group of disorders. Young and even elderly patients with symptoms related to abdominal ischaemia or peripheral vascular disease should be investigated thoroughly for hypercoagulable states and aortic pathology. Thrombosis of the aorta is generally secondary to atherosclerosis and aneurysms. Less common causes of aortic thrombosis are those related to trauma, inflammation and hypercoagulable states. These have formed the basis of several case reports. This is an analysis of the aorto-arterial thrombosis that were unrelated to atherosclerosis and aneurysms and an attempt has been made to identify the cause of such aortic thrombosis. Subjects and Methods In a span of 14 years (1986-1999), we encountered 30 cases of thrombosis of the aorta and/or its branches, unrelated to atherosclerosis. The clinical profile and autopsy findings were available in all the cases. Detailed gross examination of the heart, great vessels and their branches were carried out in all the cases. Sections from the ascending, transverse, descending thoracic and abdominal portions of the aorta, coronaries, arch vessels, visceral and iliac arteries were studied. Staining techniques included haematoxylin – eosin and elastic van Gieson in all cases, and special stains wherever required. Observation And Results There were 23 males and seven females. The ages ranged from eight to 68 years (mean 37.3 years). The majority of the aorto-arterial thrombosis (16 cases, 53%) occurred in the third and fourth decades of life. Acute abdomen and/or lower limb gangrene were the common modes of presentation of aortic thrombosis, affecting 23 patients (Table 1). Two among these presented with both. Four patients developed acute renal failure, while three cases (Cases 7, 12, 14) had no symptoms related to the thrombotic occlusion of aorta or its branches. Aorta as a source of emboli was identified in three patients. Seven patients had had features of peripheral vascular disease and three among these had undergone surgery for the same. Four other cases were diagnosed as cases of non-specific aortoarteritis. Haematological profiles were normal in all except one patient who had acute myeloid leukaemia (M1 morphology). Six were chronic smokers and five chronic alcoholics. Three had uncontrolled diabetes mellitus. Coagulation profile was studied in only one patient and was within normal limits. Heparin therapy was instituted in five. Among the 30 cases, thrombus was seen in the aorta in all but two cases (Case 2 and 7), where occlusive thrombi were restricted to major arteries (Table 2). The abdominal aorta was the site of thrombus in 14 cases, the location was supra-renal in six and infra-renal in seven. The entire abdominal aorta was involved on one patient. Thrombi in the thoraco-abdominal segment (Figure 1) were seen in three cases. Involvement of the thoracic aorta alone was seen in six; four in the proximal portion and remaining two in the distal segment of the thoracic aorta. Thrombi were multifocal in five cases (Cases 6, 19, 21, 22, 30). In the majority of the cases, the thrombi were fresh and non-occlusive. In most of the cases, involvement of the aortic branches was seen as a propagative or embolic phenomenon (Table 3). Extension of the infra-renal aortic thrombus into the common iliacs - Leriche syndrome (Figure 2) was seen in five (cases 8, 10, 19, 21, 29). Arch vessel and coronary artery thrombosis occurring synchronously with aortic thrombus was seen in one case (Case 22) and three cases (Case 8, 21 and 23) respectively. Fresh occlusive thrombosis of the major branches of the pulmonary trunk was found in six cases. One of these (Case 19) also showed aortic valvar non-bacterial thrombotic endocarditis,and two had associated pulmonary tuberculosis. Case 1 had a fresh mural right atrial thrombus. Involvement of the portal venous system occurred in two (Cases 17, 30). Considering the clinical profile and autopsy findings, we have tried to identify possible aetiologies in our cases. However, no laboratory data were available to support our findings. Nine patients were presumed to have a hypercoagulable state. One patient was a young female who had hypertension, epilepsy partialis continuans and peripheral vascular disease along with a right atrial thrombus at autopsy pointing to a possible presence of antiphospholipid antibodies. Since there was no clinical suspicion, coagulation and serologic studies were not carried out. One patient was a diagnosed case of M 1 type of acute myeloid leukaemia. He presented with bilateral acute lower limb thromboembolism, due to occlusive aortic thrombus. Section of the aortic wall revealed blast cell collection in the adventitia. Three others had uncontrolled diabetes mellitus with ketoacidosis and dehydration. Aortic atherosclerosis was mild. The thrombus in one of them (Case 4) lay over an intact fibrofatty plaque. Case 2 had an occlusive thrombus in the left subclavian artery with presence of Gram-positive cocci. No arteritis was seen. Remaining four patients were smokers, with features of peripheral vascular disease in three. Seven cases had gross and microscopic features of nonspecific aorto-arteritis. Most were stenosing lesions and had occlusive thrombi proximal to the stenotic segment with variable downward extension. The aorta in two cases showed a dense collection of lymphocytes in the adventitia with encroachment of the outer third of the media (acute aortitis-periaortitis). However, there was no destruction of the elastic lamina or fibrosis. Similar adventitial infiltrations were observed in the coeliac (Figure 3) and superior mesenteric arteries. Four cases showed marked fibrosis of the adventitia, multiple large and small areas of medial collagenisation and mild to moderate intimal fibrous thickening. Such changes resembling healed aortitis were prominently seen at the sites of thrombosis but were also seen elsewhere in the aorta and/or the branches in few cases. Inflammatory cells and obliterated vasa vasora were not seen. Healed aortic valvar infective endocarditis was encountered in one case (Case 18). Increased mucopolysaccharide deposition (Alcian blue positive) was observed in the intima and media of the aorta in a 38 year-old-male who presented with features of lower limb gangrene and acute abdomen. The histological features resembled mucoid vasculopathy, a unique vascular pathology observed in southern India. (1) Other vessels involved were left common carotid, left anterior descending coronary, coeliac and superior mesenteric arteries. Features of systemic occlusive arteriopathy (2) was observed in the coronary, superior mesenteric, left renal, splenic and inferior mesenteric arteries in a 55 year-old-man (Case 23). Multiple plaques of fresh and organising thrombi were present in the thoracic and abdominal segments of the aorta with a clinical presentation of peripheral vascular disease. The medium-sized arteries revealed severe concentric thickening of the intima by a proliferation of spindleshaped cells (Figure 4). The internal elastic lamina was intact. The media and adventitia were normal. Six cases had tuberculosis which was a sole association in two. Five patients did not have a known risk factor identified clinically or at autopsy. All were males in the third and fourth decades of life except for an elderly female. None had a previous episode of thromboembolism. One was associated with primary plexogenic pulmonary hypertension. Discussion The heart has been for long considered as a major source of peripheral thrombo-embolisrn. (3) Sometimes, aortic thrombosis can be an unsuspected source of peripheral emboli. The site is often the infra-renal abdominal aorta, especially the aortic bifurcation, secondary to complicated atherosclerosis. However, atheromas in the supra-renal abdominal aorta, (4) thoracic aorta (5) and transverse aorta (6) can also develop superimposed thrombosis. Other causes are aortic aneurysms and chronic aortic dissections. In a series of 95 cases of mural thrombus of the thoraco-abdominal aorta among 10671 autopsies by Machleder et al (7), 47 were related to aneurysmal degeneration and remaining 48 cases involved aorta of “normal calibre and configuration”. Among the latter, the authors found cases where thrombus was adherent to macroscopically near normal aorta and concluded that aortic mural thrombosis was a consequence of generalised hypercoagulation. But, these cases were not further analysed. We came across 30 cases of aorto-arterial thrombosis, unrelated to atherosclerosis or aneurysms, which prompted us to review literature for other possible mechanisms. There are many sporadic case reports and on the basis of these and our series, we were able to compile a list of causes for aortic thrombosis. Hypercoagulation of blood usually results in thrombosis in the venous circulation. Arterial thrombosis is rare; aortic thrombosis even rarer. Thrombotic episodes are a feature of anti-phospholipid antibody syndrome. Thrombosis is both venous (deep veins, vena cavae, renal and retinal veins) and arterial (cerebral, coronary, retinal and peripheral) and it is this association with arterial thrombosis which distinguishes it from all other hypercoagulable states. (8) Besides venous and arterial thrombosis, the clinical disorders in which anti-phospholipid antibodies are implicated include recurrent abortions, thrombocytoapenia, thrombo-embolic pulmonary hypertension, neurologic dysfunction and various cardiac lesions. (9-11) So far, there have been only few cases associated with aortic thrombosis, with clinical and laboratory features of primary anti-phospholipid antibody syndrome. (11-13) We presume that one of our cases (Case 1) fell into this category owing to clinical features of renovascular hypertension, epilepsy and at autopsy, the presence of thrombi in right atrium and aorta, thus involving the venous and arterial systems. However, we did not have a serologic workup. Many other blood protein defects are known to produce hypercoagulability and thrombosis such as congenital or acquired defects of anti-thrombin III, protein C, protein S, fibrinogen, heparin co-factor II and fibrinolytic pathways, (14) resistance to activated protein C (15) and prostacyclin deficiency. (16,17) Assays of the aforementioned factors require an elaborate laboratory setup (18) which may be expensive considering the circumstances of the developing countries. Five patients did not have any identifiable risk factor or an association to explain the cause of aortic thrombosis. It may be possible that they may belong to the above group or the cause is truly not known, an observation made by Wells et al. (13) Nephrotic syndrome is another cause of hypercoagulable state, again rarely associated with aorto-arterial thrombosis. (19,20) None of our patients had nephrotic syndrome. Another proved cause for venous as well as arterial thrombosis is hyperhomocystein-aemia, (21) which was not documented in any of our patients. We had a case of acute myeloid leukaemia, M1 subtype with infra-renal abdominal aortic and right pulmonary arterial thrombi in an elderly male. There is only one report of a case acute myelomonocytic leukaemia with occlusive infra-renal abdominal aortic thrombosis. (22) But this patient also had lupus anticoagulant. It is possible that the leukaemia in our case, could have induced a pro-coagulant activity, particularly since there was infiltration of the wall. In a setting of diabetes mellitus, thrombosis of the aorta usually occurs as complication of accelerated atherosclerosis. There were three uncontrolled diabetics in our series. All showed only minimal atherosclerosis. Thrombosis in them can be attributed to dehydration and ketoacidosis.23 In one of them with major arterial thrombosis (case 2), Gram positive cocci were seen in the fresh thrombus occluding the left subclavian artery. The organism may be part of a septicaemic process since the patient had extensive bronchopneumonia. However, infectious causes for aortic thrombosis have been reported especially in an immunocompromised state. (24) Hypercoagulability and venous thrombosis is a well-known association with malignancy especially gastro-intestinal and pancreatic carcinoma. There have been stray reports of aortic thrombosis. (25) None of our patients had any malignant tumour, overt or covert. Smoking is unarguably linked with peripheral vascular disease-thromboangitis obliterans. Three of the four smokers, presumed to have hypercoagulation had clinical features of peripheral vascular disease. The aorta were normal on gross and microscopic examination. Active tuberculosis was features in six patients. Four among these had other risk factors. Lang and associates (26) have demonstrated increased levels of type I plasminogen activator inhibitor and tissue factor in a 53-year-old male who underwent right upper lobectomy for tuberculosis. Fresh thrombus was seen in a segmental pulmonary artery. Arteritis was not seen. Hence with extensive progressive tuberculosis and dissemination as seen in six of our cases, systemic alterations in the above factors can tilt the balance towards a thrombotic state, especially when coupled with other risk factors. Yet, another cause of aortic thrombus reported is white clot syndrome, a rare complication of prolonged heparin therapy. (27) Among the 30 cases, five cases received heparin therapy for the thrombotic episode for only a short duration. Blunt or penetrating trauma are infrequent causes of aortic thrombosis and affect by enhanced atherosclerosis or some other condition that predisposes to thrombosis. (28-31) Trauma was ruled out in all our cases. Non-infectious inflammatory lesions of the aorta can produce narrowing or occlusion of the aortic or arterial lumens by superimposed thrombi. It has been reported with nonspecific aorto-arteritis (32) and sometimes the aortitis can be clinically occult. (33) In our series, there were seven cases where thrombosis was linked to nonspecific aorto-arteritis. The thrombi were fresh in all and occlusive in six and were proximal to the stenotic segment. Two cases showed a dense adventitial infiltrate of lymphocytes with a spill-over into the outer-third of the media. This lesion represents early, occult aortitis. Features of healed occult aortitis, peri-aortitis (adventitial fibrosis, medial scarring and intimal fibrous thickening) were observed in four cases. Vasa vasora were patent and there were no inflammatory cells. Cause for the aortitis in one of them could be attributed to infective aortic valve endocarditis. Similar changes can be produced by obstruction of vasa vasora. (34) One wonders therefore whether there could have been fleeting occlusive thrombosis of these small vessels and subsequent alterations in the aortic wall produced by ischaemia. Case 22 was a 38-year-old male with a long segment thoracoabdominal thrombosis with features of mucoid vasulopathy. This entity was described by Sandhyamani from Kerala, affecting young males belonging to low socioeconomic strata. (1) There is accumulation of mucopolysaccharides in arteries, veins, fascia, vasa vasora as well as organ connective tissue and depending upon the severity of the deposition, patients were categorized into two groups, Group 1 and Group 2. Our case fell into group 2 where deposits were less severe. Thrombosis has been described in muscular and musculo-elastic arteries in mucoid vasculopathy, but occurred in the aorta in a setting of aorto-arteritis. (1) Systemic occlusive arteriopathy was a term coined by Siegel et al (2) to describe fibromuscular dysplasia affecting many vessels. Fibromuscular dysplasia is a segmental, non atherosclerotic vascular disease of unknown aetiology, presenting typically between the second and fourth decades of life. (35) Mainly renal arteries are involved, but other vessels can also be affected. It has been classified as intimal fibroplasia, medial fibromuscular dysplasia and periarterial fibroplasia. (36,37) Our case had intimal fibroplasia involving all the coronary arteries and four splanchnic arteries and is unique because of its association with multifocal aortic thrombosis which has not been reported earlier in literature. An atherosclerotic plaque with an intact fibrous cap is usually not thrombogenic unless accompanied by its complications. However, changes related to age such as elastic fibre fragmentation and cystic medionecrosis can cause aortic dilation and stress-induced fracture of an uncomplicated plaque. Exposure of thrombogenic components then leads to thrombosis, as reported by Nader et al. (38) All our cases, surprisingly, had only minimal atherosclerosis, including the elderly and the diabetics. Thrombi were found over an intact fibrofatty plaque in cases 4 and 20. However, no degenerative age- related changes were seen. Besides, these cases had other risk factors. Thus, non-antheroscleroctic aortic thrombosis is a heterogeneous group of disorders and young patients and even elderly with symptoms related to abdominal ischaemia or peripheral vascular disease should be investigated thoroughly with complete haematological, coagulation and serological profiles. Early diagnosis is essential to treat such patients. References
© Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01002f4.jpg] [jp01002f3.jpg] [jp01002f1.jpg] [jp01002t1.jpg] [jp01002f2.jpg] [jp01002t3.jpg] [jp01002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}