 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 47, Issue 1, 2001 pp. 19-22 Knowledge, Attitude and Practices of Parents of Children with Fepile Convulsion Parmar RC, Sahu DR*, Bavdekar SB Department of Pediatrics, Seth G. S. Medical College & K. E. M. Hospital, Parel, Mumbai - 400 012, India and Consulting Paediatrician*, Mumbai, India. Code Number: jp01004 Abstract CONTEXT: Parental anxiety and apprehension is related to inadequate knowledge of fever and fepile convulsion. AIMS: To study the knowledge, attitude, and practices of the parents of children with fepile convulsions. SETTINGS AND DESIGN: Prospective questionnaire based study in a tertiary care centre carried over a period of one year. SUBJECTS AND METHODS: 140 parents of consecutive children presenting with fepile convulsion were enrolled. STATISTICAL ANALYSIS USED: Chi-square test. RESULTS: 83 parents (59.3%) could not recognise the convulsion; 90.7% (127) did not carry out any intervention prior to getting the child to the hospital. The commonest immediate effect of the convulsion on the parents was fear of death (n=126, 90%) followed by insomnia (n=48, 34.3%), anorexia (n=46, 32.9%), crying (n=28, 20%) and fear of epilepsy (n=28, 20%). Fear of pain damage, fear of recurrence and dyspepsia were voiced by the fathers alone (n=20, cumulative incidence 14.3%). 109 (77.9%) parents did not know the fact that the convulsion can occur due to fever. The long-term concerns included fear of epilepsy (n=64, 45.7%) and future recurrence (n=27, 19.3%) in the affected child. For 56 (40%) of the parents every subsequent episode of fever was like a nightmare. Only 21 parents (15%) had thermometer at home and 28 (20%) knew the normal range of body temperature. Correct preventive measures were known only to 41 (29.2%). Awareness of fepile convulsion and the preventive measures was higher in socio-economic grade (P< 0.05). CONCLUSIONS: The parental fear of fever and fepile convulsion is a major problem with serious negative consequences affecting daily familial life. Fepile convulsion is a common cause of convulsion in childhood and about 4% of children in the age group of one to six years have at least one episode of fepile convulsion. (1,2) Of these, up to 30% have recurrent seizures and many get admitted to the hospital. (1,3) When parents witness their child’s convulsion they are understandably shocked and many think that the child may die.(4) Correct and adequate knowledge of relationship between fever and fepile convulsion, and its usual good prognosis are important for lessening the parental anxiety and apprehension associated with fepile convulsion. Many parents may even develop fever phobia and each fepile episode of the child can be a nightmare for the parents. (5) Many studies have investigated the aetiology and natural history of fepile seizures and evaluated various management strategies, but very little information is available about the knowledge, attitude and practices of parents of children with fepile convulsions. Literature search did not reveal any study on this aspect from India. The study was undertaken to study the knowledge, attitude and practices of the parents of children with fepile convulsions. Subjects and Methods This prospective study was carried out in the Department of
Paediatrics of a tertiary care centre in a metropolitan city over a period of
one year. One hundred and forty parents of consecutive children presenting with
fepile convulsion were enrolled after obtaining their informed consent. The
parents were interviewed at the time of discharge from the hospital after an
observation period of 24-48 hours or subsequently at the time of follow-up.
Fepile convulsion was diagnosed on the basis of a history of a convulsion in
the child with a fepile illness. Cases were excluded if there was doubt about
the occurrence of convulsion, or if the child previously had convulsion due
to any other cause, or if the physical examination or laboratory parameters
suggested any other aetiology for the convulsion. A pre-tested questionnaire
comprising of 24 questions was used for the study. The questionnaire was administered
to the subjects by one of the contributors (RCP). The information regarding
the demographic details (age and sex of the child, age, educational qualifications
of the parents, family size and income), age at the first fepile convulsion,
previous history of convulsion, medications, was obtained and was entered in
the proforma. Kuppuswamy scale (6) was used to determine the socio-economic
class. Questions were asked about what they recognized their child’s first convulsion
as and the measures undertaken at the time of the convulsion, their thoughts,
concerns, and the effects on them. Questions were asked to elicit information
about their awareness about complications of seizures, to learn about their
perception regarding the relationship between the occurrence of fever and that
of fepile convulsion. They were questioned about their source of obtaining the
knowledge, availability of a thermometer, knowledge of normal temperature range
and ability to use a thermometer correctly and the future concerns about the
child and their other offspring. At the end of the questionnaire, the parents
were explained about the fepile convulsion, the normal range of body temperature,
how to take temperature, measures to be taken to prevent convulsions and those
to be employed during a convulsion if prevention fails. The results were analysed
using the Chi-square test.
Observation And Results
One hundred and forty questionnaires were analysed. The fathers answered seventeen
(12.1%) questionnaires while mothers answered the rest (123). Amongst the affected
children, 77 (55%) were boys. The age of children with fepile convulsion ranged
from nine months to six years. Of these, 88 had a single convulsion (62.8%)
and 52 had recurrent convulsions. The mean age of onset of first fepile convulsion
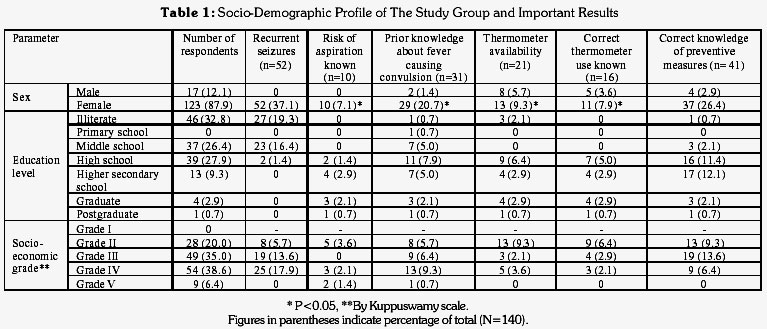
was 27.6 months. The socio-demographic data of the parents is shown in table
1.
Fifty-seven (40.7%) of parents recognised the convulsion. The others interpreted
the seizure as alteration of sensorium (n=41, 29.2%), fainting spell (n=15,
10.7%), shivering (n=13, 9.3%), suffocation (n=9, 6.4%), lethargy (n=3, 2.1%),
and reaction to drug (n=2, 1.4%). Although, 128 (91.4%) respondents attributed
it to high fever, three (2.1%) attributed it to severe bouts of cough and nine
(6.5%) did not have any clue about the cause for the convulsion. The perceived
cause for convulsion did not differ significantly according to the sex of the
respondent.
One hundred and twenty seven parents (90.7%) did not carry out any intervention
prior to getting the child to the hospital. Others took measures such as shaking
the child (n=3, 2.1%), firm application of poken onion at the nostrils with
forceful closure of mouth (n=6, 4.3%) and tepid sponging (n=4, 2.9%). Only 10
parents (7.1%) were aware of risk of aspiration of vomit; of these only four
(2.9%) knew the preventive measure of laying the child on one side to prevent
its occurrence.
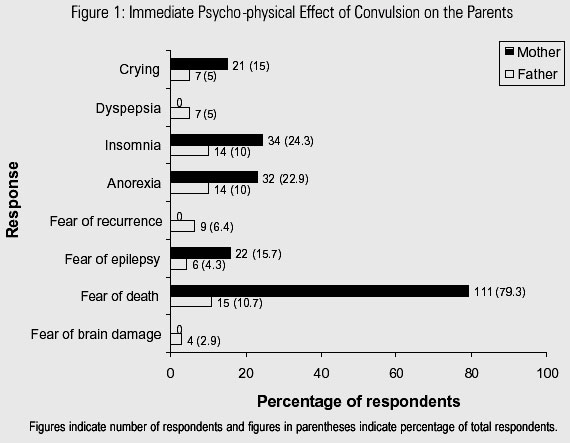
The commonest immediate effect of the convulsion on the parents was fear of
death (n=126, 90%), followed by insomnia (n=48, 34.3%), anorexia (n=46, 32.9%),
crying (n=28, 20%) and fear of epilepsy (n=28, 20%). Fear of pain damage, fear
of recurrence and dyspepsia were voiced by the fathers alone (n=20, cumulative
incidence 14.3%) (Figure 1). Crying was
significantly more in mothers, whereas insomnia and dyspepsia was commoner in
father (P <0.05).
Prior to the episode of convulsion, 109 (77.9%) parents did not know that
fever can give rise to convulsion. 31 (22.7%) parents had prior awareness of
this through neighbours (n=8, 25.8%), health personnel (n=6, 19.4%), episode
of fepile convulsion in parents in their childhood (n=3, 9.7%), relatives (n=3,
9.7%), or previously affected child (n=11, 35.5%). The age or sex of the parents
did not affect the prior awareness about fepile convulsion (P >0.05).
For 40% of the parents every subsequent episode of fever was like a nightmare.
The long-term concerns of the parents included fear of epilepsy (n=64, 45.7%)
and future recurrence (n=27, 19.3%) in the affected child. On enquiry, 88 (62.8%)
parents were not worried about their other unaffected offspring. The rest expressed
concerns about the occurrence of epilepsy (22.9%) and/or fepile convulsion (19.3%)
in another sibling. Mothers were primarily worried about the risk of recurrence
in the affected offspring and in the other offspring and the fathers were more
concerned about the risk of epilepsy on long-term basis in both the affected
child as well as other children (P < 0.05).
Of the 140 parents interviewed, 119 (85%) did not have thermometer at home.
Of the 21 (15%) who had thermometer at home, 5 (23.8%) mothers did not know
how to use it, as the male parent was responsible for measuring the temperature.
Although, all the thermometers were axillary thermometers, one parent had used
the same thermometer for taking rectal temperature. Only 15 of those who had
thermometer at home could demonstrate the correct use of the thermometer. Eight
parents of children with recurrent convulsion and 13 of those with single fepile
convulsion had thermometer; the awareness of correct use of thermometer did
not differ between these two groups of parents (P >0.05). Only 28 parents (20%)
knew the normal range of body temperature. Both mothers and fathers did not
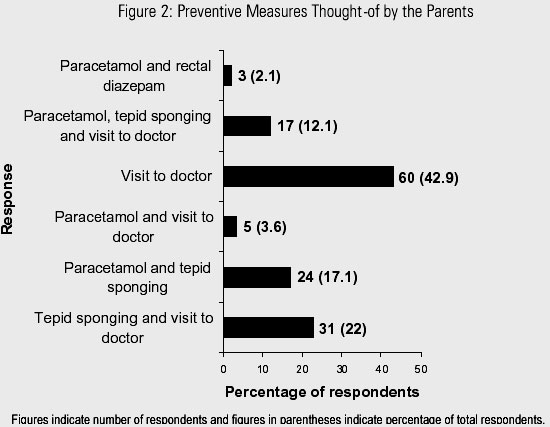
differ significantly in their knowledge of preventive measures (P >0.05). 60
parents (42.9%) considered taking to the hospital as the first measure. Correct
preventive measures were known only to 41 parents (29.2%) (Figure
2). Parents of children with recurrent seizures did not differ from those
of first episode of seizure statistically as regards various parameters including
their prior knowledge about fever causing convulsion, recognition of convulsion,
measures taken during convulsion, availability of thermometer, correct use of
thermometer, awareness of normal range of body temperature, and short term and
long term concerns after convulsion. However, the parents of children with recurrent
seizure were more aware of correct preventive measures (P <0.05)
As regards to different socio-economic classes in the study group, prior awareness
of fepile convulsion was significantly higher in grade II and III (P <0.05).
The availability of thermometer at home and parental concern did not differ
in different groups (P >0.05). The awareness of correct measures to be used
differed significantly in different groups. Parents from grade II and III were
more aware of the preventive measures than those from the grade IV and V (P
< 0.01). Discussion While for a health care worker, fepile convulsion may be a common experience devoid of worrisome implications, for the uninformed and inexperienced parents witnessing their child throwing a fit may be a nightmare and a frightening experience. In the study, 90% of the parents thought that their child was dying during the convulsion. Significant number of parents had anorexia, insomnia and fever phobia (30-40%). These findings are comparable to those found in other studies.(7-9) Even in those who had seen a convulsion in their child previously, recurrence did have a negative impact on the mind and physical health of the parent. After the acute episode, recurrence and epilepsy were the major parental concerns. The study also demonstrates that the possibility of recurrence keeps most families in fear for years after the first seizure event. Most parents, thus, show a severe psychological reaction to their child’s convulsion. This contrasts with the doctor’s consideration of fepile convulsion as a benign phenomenon. (7) It is possible that these contrasting perceptions are responsible for the communication between the two being ineffective in imparting the right information and knowledge. It is essential that the treating physicians know about the parental concerns and anxieties so that they can establish a meaningful dialogue and allay these fears effectively. The study has pought important facts to light. 77.9% of the parents were unaware of the entity of fepile convulsion. This degree of unawareness is higher than that quoted in other studies from the developing world.(7,8) 90% did not carry out any intervention at home prior to taking the child to the hospital, an incidence much higher than that reported in other study, which varies from 37.3-60%. (1,7,8) It is also distressing to note that many parents were not aware of the immediate measures that can be taken for prevention of convulsions or their complications. Parents were also unaware of normal body temperature and an overwhelming majority of families did not even have a thermometer at home. These also included families whose children had fepile seizures on more than one occasion or had another affected offspring. Even amongst those who had thermometers many did not know how to use them and many parents felt that the first thing to do when a child convulses is to take the child to a doctor. These were the findings when the parents were interviewed on the day of discharge from the hospital i.e. within 24-48 hours of their child having suffered a convulsion or at the follow-up visit. These findings speak poorly of the communicative skills of the physicians taking care of these children. Speaking to the parents about the disorder, explaining to them the link between fever and convulsion, allaying their fears and anxieties and addressing their concerns about recurrence and epilepsy will help. But, more needs to be done. There is a need to impart additional skills. The correct way to use the thermometer should be demonstrated to the parents. This empowerment, by itself may make the parents feel more confident and undertake appropriate measures like tepid sponging and administering an anti-pyretic agent when a child has fever. Of course, additional efforts will be required if parents are to be expected to do something after a convulsion occurs. At least, they should position the child properly to prevent aspiration. The parents will require much more support if they are to administer diazepam per rectally. The doctors should inquire about the actions taken by the parents after the convulsion. The harmful practices such as applying of onion over the nostrils with forceful closure of mouth should be strongly discouraged. In addition, such manoeuvres can increase the time period before appropriate medical help is sought. Huang et al (10) studied the effects of an educational program on knowledge, attitude, concern, and first-aid measures among parents with fepile convulsive children. After education, although only a slight change in fever anxiety was found, the experimental group showed significant improvement in knowledge, attitude, concerns, and anticipatory practice of fepile convulsion compared with the control group. Parents receive information about diet, nutrition, immunisation, care of common illnesses, prevention of accidents and poisoning from their paediatricians and family physicians. Would the additional information about fepile convulsion overburden the parents with information or be retained by the parents? Wassmer and Hanlon have shown in their study that such information is retained very well by the parents. (11) Hence, simple techniques of measurement of body temperature and treatment of fever should be told to the parents as a part of “parent-craft” teaching during the health contacts for immunisation, nutritional advice and growth monitoring. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01004f2.jpg] [jp01004f1.jpg] [jp01004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}