 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 47, Issue 1, 2001 pp. 52-53 Myxoid Liposarcoma of the Spermatic Cord Kashid YS, Bakshi
GK, Joshi AS,* Mohite JD
Department of General Surgery and
Pathology*, Seth G.S. Medical College & K.E.M. Hospital, Parel, Mumbai - 400
012, India. Code Number: jp01002 Case History An 80-year-old man
presented with a rapidly increasing swelling in the left inguinoscrotal region
of three months’ duration and a lump on the same side of lower abdomen, since
two months.
On examination, the patient had
hard, immobile, retroperitoneal lump continuous with left cord structures. Computerised
tomographic (CT) scan showed a well defined inguinoscrotal mass of mixed density
(soft tissue and fat attenuation) extending into pelvis and left side of retroperitoneum
upto the lower pole of the left kidney, without associated lymphadenopathy.
The diagnosis was liposarcoma of spermatic cord with extension into retroperitoneum.
Search for metastases in lungs and liver did not reveal any.
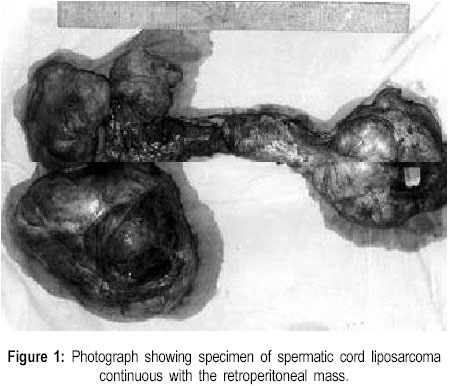
At laparotomy, we found a large,
well-encapsulated and hard tumour in the left retroperitoneum, pushing the bowel
loops, bladder and left ureter towards right side and it was continuous with
the left inguinoscrotal swelling. The testis was separate and normal. The aorta
and IVC were free from the tumour. Complete excision of the retroperitoneal
and inguino-scrotal tumour with left orchidectomy was done (Figure
1).
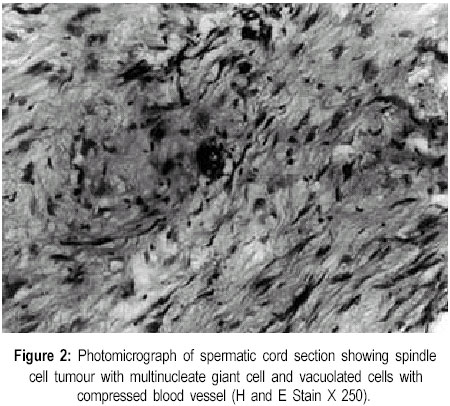
Microscopically, it showed a highly
cellular spindle cell tumour with variegated appearance showing fascicles, loose
myxoid areas and poorly cellular areas. There were many multinucleate tumour
giant cells, lipoblasts, stellate cells and compressed vascular channels. Frozen
section and Oil Red O stain showed abundant fat in the tumour cells (Figure
2). Histopathological diagnosis was myxoid liposarcoma of the spermatic
cord with extension into retroperitoneum. In our patient though complete excision of the tumour was possible, we could not get wider margin for radical excision. Hence, the patient was advised postoperative radiotherapy. The patient had local recurrence and liver metastasis within three months and succumbed later. Discussion Myxoid liposarcoma is rarely found in the spermatic cord. It tends to occur in the elderly, presenting as painless scrotal swelling and is often confused with hydrocele or chronic incarcerated inguinal hernia. (1) Till 1997, only 14 cases of myxoid liposarcomas have been reported. (2) Of these one was a giant tumour weighing 42 kg. (3) This tumour may arise from the cord tissue representing extension of retroperitoneal fat or as malignant transformation of a preexisting lipoma. It generally behaves like a well differentiated liposarcoma.1 CT scan is diagnostic of liposarcomas. Wide excision with orchidectomy is the treatment of choice for spermatic cord liposarcomas. Local recurrence is commoner than distant metastasis. (4) Retroperitoneal lymphadenectomy is not recommended as retroperitoneal lymph nodal spread is unlikely. (5,6) Adjuvant radiotherapy is recommended in well-differentiated and myxoid type if local control is not complete. This may reduce the incidence of locoregional recurrence. (7) Benefit of chemotherapy is controversial. (4) Myxoid liposarcoma of the spermatic cord being a low grade, well-differentiated sarcomas it does not recur with a higher grade or in less-differentiated form.1 Local recurrence is best treated by wide excision, but the prognosis is poor. (8) References
© Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01015f2.jpg] [jp01015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}