 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 47, Issue 1, 2001 pp. Neurobiological Correlates of Panic Disorder and Agoraphobia Al-Haddad MK*, Sequeira RP**, Nayar U*** Department of Psychiatry,* Salmaniya Hospital; Departments of Family and Community Medicine,* Pharmacology and Therapeutics,** Physiology,*** Arabian Gulf University, P O Box 22979, Bahrain. Code Number: jp01017 Abstract Panic
Disorder and agoraphobia offer considerable diagnostic and management challenges,
particularly in general practice. We describe a typical case of panic disorder
in a young adult. The recent advances in our understanding of brain functions
can be used to explain to a certain extent the biologic basis of panic disorder.
A hypothetical model integrating current views on panic disorder and agoraphobia
has been proposed. The management principles including the role of cognitive
therapy and pharmacotherapy have been discussed.
Since the time of the ancient Greeks, there have been consistent reports of
a disorder causing the most irrational fear in otherwise sane people. In the
6th century BC the Greek poetess Sappho gave a clear description of the symptoms
of panic: dry mouth, a sense of burning under the skin, a sense of being about
to die, tinnitus, blurred vision and sweating. It was not until the later part
of the nineteenth century that this came to be known as “agoraphobia”, which
literally translates “fear of the market place”. More recently the term is used
to mean fear of public places or open spaces. While such fears characterize
the majority of agoraphobics, recent evidences suggest that these situational
fears are not the primary fears in agoraphobia. It is the fear of panic attacks
regardless of where they occur that is the primary fear in panic disorder and
agoraphobia. When panic attacks are very frequent or when a person spends a
considerable amount of time fearfully anticipating the next attack of panic,
that individual is said to suffer from panic disorder. The DSM – IV classification (1) defines a panic attack as a discrete period of intense fear or discomfort, with four or more of the following symptoms:
Agoraphobia
is defined as “anxiety about being in places or situations from which escape
might be difficult (or embarrassing) or in which help may not be available in
the event of having an unexpected or situationally predisposed panic attack
or panic like symptoms”. (1) Characteristically situations that are avoided
include traveling alone, being outside home alone, in a tunnel or open spaces. Case Report The following case illustrates the salient clinical features of panic disorder: A 29-year-old male came to the psychiatric clinic after watching a programme on the local TV addressing panic disorder. For the past two years, he has undergone different medical investigations and consultations, including one with a cardiologist because of his belief that he has a heart problem. Two years ago, while
he was presiding a stormy meeting of his company’s board, he felt dramatic increase
in his heart rate, his breathing became difficult, he felt tingling sensations
in the fingers of the left hand with trembling. He also developed intense stabbing
pains in the chest, profuse sweating and muscle stiffness. He felt that he might
be having a heart attack. He was rushed to the emergency department where an
ECG was recorded and serum cardiac enzymes were tested. No abnormality was detected
and he was soon released after an i.v. injection of 10mg diazepam. He was advised
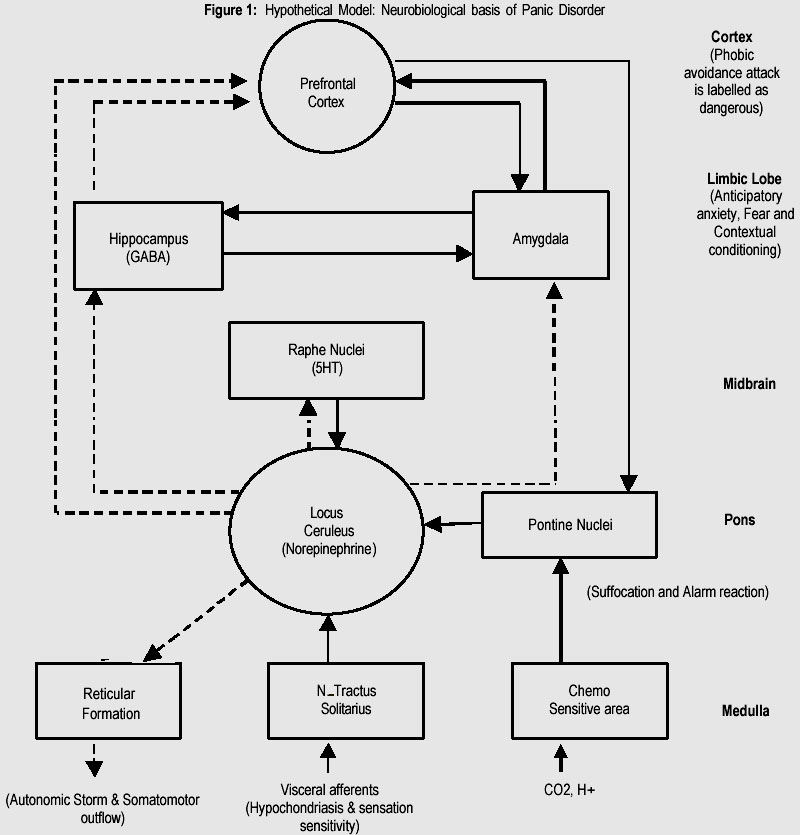
to check with his general practitioner (GP) later on. Following his first attack he would never go on his own to any place where medical help could not be quickly obtained. In fact he limited traveling in his car alone to a radius of 3-4 km only around the emergency department in order to reach help in case he develops a heart attack. He started to avoid closed places like cinemas and shopping malls anticipating that his escape route might be blocked; he gave up altogether his hobby of fishing in his boat because it would be too far and too late to seek medical help. Born and raised in a small city, he left school to attend college in USA to study Business Administration. He is the youngest of four children, with an older brother and two sisters. Both parents are alive and well; mother was described as overprotective and a worrier. None of his direct family members had contact with psychiatric services. After finishing his studies he worked for four year with his father who is a businessman. Later, he established his own company and managed it successfully for nearly three years. He is not married and remained with his parents at home. He does not smoke or drink, he does not have a girl friend or a current emotional attachment. His GP did a routine physical check-up, full blood count and thyroid function tests and detected no abnormalities. He was advised to cut down daily consumption of Turkish coffee. He treated him with diazepam 5mg tid. The cardiologist started him on propranolol 40mg tid. His symptoms were relieved but still recurred once or twice a month. Discussion Before a diagnosis of panic disorder is established one must exclude other causes of anxiety e.g. hyperthyroidism, Cushing’s syndrome, phaeochromocytoma, hypoglycemia, vestibular disturbances and mitral valve prolapse syndrome. Differentiation from other psychopathologic conditions can at times be problematic and include many anxiety disorders such as social phobia (panic is consequence of fear of scrutiny by others, or negative evaluation), separation anxiety (mainly in children), claustrophobia (being in an enclosed space and unable to get out causes the person to panic), while in agoraphobia the individual fears he might have a panic attack in an enclosed space because of inability to get out easily. This case illustrates three observations common to panic disorder and agoraphobia. First, the disorder had a clear onset, which the patient has dated back to his first attack of panic. Second, the avoidance of situations developed subsequent to the panic attack for the fear of the consequence of having a heart attack. The panic attack involved a dramatic increase in sympathetic arousal, the origin of which is not clear to the patient and subsequently misinterpreted as a sign of a heart attack. Most phobias emerge in childhood and early adolescence except for agoraphobia and claustrophobia, which emerge after adolescence. (5) It was initially hoped that there is a unique predisposition to panic attacks. The genetic studies implied a heritable component to panic attacks. (6,7) However, it was explained that the hereditary predisposition was a general trait of anxiety proneness rather than being specific to panic disorder or agoraphobia. (8,9) Another explanation to increased vulnerability implied that the flight or fight response is more easily triggered. (10) This response may be triggered under potentially dangerous circumstances (true alarm), or it may be triggered in the absence of potential danger in response to a negative perception of stress (false alarm). When symptoms overlap between patients with panic disorder, overlap was more obvious among those with panic and generalized anxiety disorder. In spite of the fact that an anxiety response is more easily triggered in a person with anxiety proneness, there has been no clear evidence of a biological substance causing panic disorder. Hence more attention was directed to the factors that predispose an individual with anxiety traits towards developing panic disorder and agoraphobia. Hyperventilation was one of the factors exclusively scrutinized in order to find out whether it can cause or exacerbate a panic attack. In addition, cognitive process has been extensively studied. The symptoms of hyperventilation syndrome were found to be very close to those of panic attacks. This has consequently lead to the assumption that hyperventilation can be blamed for the triggering of panic attacks or at least contribute to their exacerbation in susceptible individuals. The support for this hypothesis is the finding that patients with panic attacks recognize the symptoms produced by voluntary hyperventilation as similar to the symptoms of panic. (11,12) However, other findings were not consistent with the hypothesis: while panic attacks induced by lactate infusion were associated with hyperventilation, voluntary hyperventilation did not produce a clear panic attack. (13) Furthermore, no difference was found between the symptoms of panic attacks with or without hyperventilation. (14) This leads to the conclusion that although hyperventilation can produce symptoms similar to panic attacks, it is not the cause. The obvious question that naturally follows is how do the symptoms produced by hyperventilation relate to the experience of panic attacks? Various experimental
models have been used in exploring the neural substrate and neurotransmitters
involved in panic disorder. The patient seems to experience a crescendo of autonomic
symptoms and then fears of impending death. (15) Based on accumulated experimental
evidence the irritable foci in the brain stem, especially the pons (locus coeruleus)
and medulla (chemoreceptors), serve as the source of panic with characteristic
hyperventilation and cardiovascular changes. It has been proposed that patients
with panic disorder inherit brainstem loci that are hyperexcitable, and that
aberrant neural transmission excites these loci. (16) Asymmetry in blood flow through specific limbic structures, (15) especially cholecystokinin (CCK-4) induced changes in regional cerebral blood flow. (20) during panic attacks has been extensively investigated. The temporal dynamics of CCK-4 induced changes in blood flow suggests activation of brainstem-hypothalamic region leading to claustrum-insular activation. (21) In addition, studies on cerebral metabolic activity by positron emission tomography scan in panic disorder have shown aberrant metabolism in hippocampal and parahippocampal regions. (22) Whether this abnormality represents altered blood flow, a change in neuronal activity or output from these areas is uncertain. The hippocampal formation with its connections to the amygdala may also play a role in contextual conditioning. (23) This form of conditioning to a “place” or “situation” in which external stimuli become associated with fearful behaviour is relevant in panic disorder and agoraphobia. (24) An integrated neurobiological model in which fear and anxiety act as a backdrop for explaining panic has been suggested: (25) the structures and pathways involved in transmission of sensory data to signal processing areas in the cortices, limbic areas (amygdala, hippocampus), and brain-stem structures (periaqueductal grey area, locus coeruleus) are included in this integrated model. Once a threat or fearful stimulus is assessed through a process of integrating past and present experiences, the processing areas (orbitofrontal cortex, amygdala) formulate and elicit a fear or anxiety response. Key structures that execute the response include the locus coeruleus (triggering autonomic and neuroendocrine responses via the hypothalamus and nucleus paragigantocellularis), the hypothalamus (autonomic and neuroendocrine components of fear response), dorsal nucleus of the vagus (parasympathetic activation), parabrachial nucleus (fear-induced hyperventilation), trigeminal nucleus and facial motor nucleus (facial expression of fear), and striatum and periaqueductal grey area (fear induced motor activation for fight or flight responses). (26,27) Currently available experimental evidence explaining the neurobiological basis of panic disorder, including the neuroanatomic pathways with their connections are summarized in Figure-1 (Fig. not available). The major neurotransmitter involved in some of these loci – norepinephrine in locus coeruleus, 5-hydroxytryptamine (5HT) in raphe nuclei, and gama aminobutyric acid (GABA) in the hippocampus – can be correlated with therapeutic response to drugs such as central sympatholytics (clonidine), serotonin selective reuptake inhibitors (SSRI) and benzodiazepines, respectively. (28,29) While the proposed hypothetical model is an oversimplification, it helps in formulating a convergent view of the clinical features of panic disorder derived from advances in neurobiology. Various cognitive models have explained ways in which the cognitive processes can contribute to the production of panic attacks. Figure-1 emphasizes the catastrophic misinterpretation placed upon internal bodily cues in some individuals with anxiety sensitivity. (30) Fear of these internal sensations may form a crucial maintaining factor in panic disorders: when these sensations are experienced they can elicit panic reactions since the feared interceptions are usually associated with anxiety, one may expect the panic reaction to exemplify the feared situations. The panic attack can thus be conceptualized as a positive feedback loop, the panic disorder as a fear or phobophobia. (31) Anxiety traits may predispose individuals to “false alarms” but anxiety sensitivity may encourage an individual to worry about the sensations. In other words the development of panic attack is not the experience of somatic sensation, but the interpretation placed upon those sensations. In support of this notion it was found that agoraphobics interpret ambiguous scenarios in a more threatening manner than normal subjects. (32) In addition there is bias towards threat-related information leading to superior recall of phobic material when compared with normal subjects. (33) Panic disorder and agoraphobia are currently conceptualized as two separate, but frequently related, disorders. Panic attacks are in a way the motor that drives the agoraphobic avoidance. Therefore, it is expected that effective treatment of agoraphobia requires effective management of panic attacks. The first goal of an effective treatment for agoraphobia (with panic disorder) is to stop the panic attacks and their effect on the patient’s life. The second goal is to reduce any concurrent agoraphobic avoidance which usually involves anticipatory anxiety and anxiety triggered upon exposure. In short, effective treatment of panic disorder and agoraphobia should be based on three elements namely control of panic attacks, the cessation of fear-driven avoidance and the reduction of the vulnerability. The first method used for treatment is cognitive therapy which is based on the cognitive theory of panic. Typically cognitive therapy is focused on eliminating the catastrophic interpretation of the panic symptoms. Various techniques are used to help patients identify, then change the misinterpretations of their bodily sensations. (34) Cognitive procedures include identification and challenge of the patient’s evidence for his / her misinterpretations, and replacing them with the realistic ones. This includes induction of panicky sensations by hyperventilating the patient in order to demonstrate possible causes of the patient’s symptoms. A home work assignment is given in which the patient keeps daily record of negative thoughts and irrational responses. Applied relaxation devised by Ost, (35) is a behavioural approach used for teaching patients to identify early signs of panic and later on controlling them through relaxation techniques. Several classes of
drugs have been used with variable degree of success in the management of panic
disorder and agoraphobia: antidepressants including the tricyclic drugs, serotonin
selective re-uptake inhibitors (SSRI) and monoamine oxidase inhibitors (MAOI),
as well as antianxiety drugs like benzodiazepines. Benzodiazepines have a rapid
onset of effect and are effective in blocking anticipatory anxiety as well as
panic attacks. The main limitations of benzodiazepines such as alprazolam, clonazepam
and diazepam, is their ability to cause excessive sedation, drug-dependence,
memory problems, falls in the elderly and occasionally, paradoxical rage. A
gradual tapering of the dosage is required to minimize the severity of withdrawal
symptoms. (36,37) Concurrent use of benzodiazepines and psychotherapy for panic disorder is a prevalent but highly controversial practice. Cognitive behavior therapy has been combined with pharmacotherapy in the treatment of panic disorders in three ways: (a) to treat agoraphobic symptoms in the condition of panic with agoraphobia; (b) to reduce withdrawal effects during drug-taper, and (c) to treat panic attacks. (40) Efforts to educate and counsel patients in the clinical setting regarding the psychopathology of panic attacks may improve the outcome of pharmacotherapy. Since the cognitive behaviour therapy involves usually several sessions, it is not widely offered to patients because of cost considerations. Although there are many rationales for combining pharmacotherapy with psychotherapy approach, critics contend that benzodiazepines foster drug abuse and dependence and undermine psychosocial treatment. (42) However, pre-existing pharmacotherapy with either antianxiety or antidepressant drugs did not either enhance or detract the long-term outcome of brief intensive group cognitive behaviour therapy in patients with panic disorder with or without agoraphobia. (42) Since panic disorder with or without agoraphobia is a prevalent condition which presents primarily in general practice, a recent study looked into the effectiveness of fluvoxamine or cognitive behaviour therapy either alone or in combination, in a general practice setting. All modalities of therapy showed a satisfactorily significant advantage over placebo as regard to a range of outcome ratings. Interestingly the group employing cognitive behaviour therapy showed the most robust and consistent response. (43) Although improvement during treatment is well documented in patients with panic disorder and agoraphobia, a recent study has confirmed lasting improvement years after exposure treatment, though some residual symptoms were the norm. (44) The availability of SSRI such as fluoxetine, fluvoxamine and setraline has shifted the emphasis from tricyclics in the treatment of panic disorder. These drugs are better tolerated by patients and the drop-out rates are generally low. In two multicentric trials. (45,46) the efficacy and safety of sertraline was confirmed. Further data supporting the clinical preference for SSRI are emerging. In clinical settings, the administration of a benzodiazepine with a tricyclic has also been proposed to reduce the frequency and severity of adverse effects in the treatment of panic disorder. Usually these patients may require a dose of imipramine in excess of 125 mg/day, a dose at which significant adverse effects are expected to occur. Combination of imipramine with lorazepam showed that in almost three fourth of these patients the panic attacks disappeared and were free from phobic attacks. Such combined treatment allowed the use of low doses of drugs, reduced the frequency and severity of the adverse effects and improved patient compliance. (36) The MAOI are believed by some clinicians to be most potent anti-panic agent, but their considerable adverse effects limit their use. (47) The availability of selective MAOI offers a new avenue in evaluating their potential in treating panic disorder. The beta adrenoceptor blocking agent propranolol is mainly useful for ameliorating the autonomic-sympathetic component of a panic attack, particularly the palpitations and tremors. In addition, to what extent the central effects of propranolol contribute towards the clinical benefit is uncertain. Based on the data drawn from the Cross-National Collaborative Panic Study, over 70% of the patients used primary care for mental health services, whereas about 47% of the patients used specialty mental health services. Nearly half of the patients saw a non- psychiatrist medical specialist, most often a cardiologist. The mean estimated expenditure for the panic episode was $ 3339, about half of which was accounted for by specialty mental health expenditures. (48) Both primary care and specialty mental health sectors play prominent roles in the community treatment of panic disorder. Conclusion During the past decades substantial progress has been achieved in our understanding of panic disorder and agoraphobia, A case of panic disorder with agoraphobia described in this paper illustrates the typical course of events likely to occur in a general practices setting. We have reviewed some recent advances in neurobiology of panic disorder and agoraphobia and have proposed a hypothetical model which helps in formulating a convergent view of the clinical features of panic disorder and agoraphobia. The various modalities of treatment incorporating cognitive therapy and pharmacotherapy have been discussed. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01017f1.jpg] |
| |||||||||

{kind=link}