 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 47, Issue 2, 2001 pp.116-118 Diffuse Calvarial Meningioma: A Case Report Muzumdar DP, Vengsarkar
US, Bhatjiwale MG, Goel A
Department of Neurosurgery, Seth G.S. Medical College
and King Edward VII Memorial (K.E.M.) Hospital, Mumbai and Department of Neurosurgery,
Sir Hurkisondas Nurrottamdas Hospital and Research Centre, Mumbai Code Number: jp01035 Abstract A rare case of a
diffuse calvarial meningioma in a sixty-three year-old female is reported. The
patient presented with headache, painful proptosis and chemosis of the left eye.
Imaging showed that the frontoparietal calvarium on both sides and the left orbital
roof were thickened. The thickened bone showed patchy rarefaction. In relationship
to the thickened bone, there was an enhancing en-plaque meningioma. The tumour
extended on to the superolateral aspect of the left orbit and resulted in proptosis.
Excision of the left frontoparietal calvarium and the orbital tumour was performed.
The management of diffuse calvarial meningioma is discussed and the relevant literature
is piefly reviewed.
Key Words:Meningioma, En-plaque,
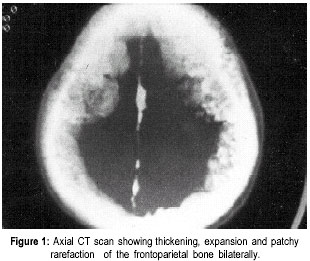
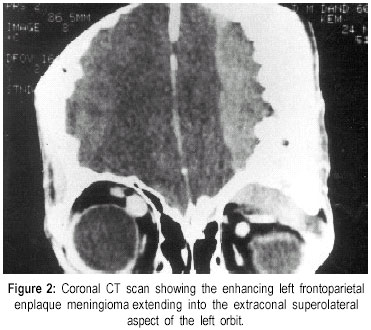
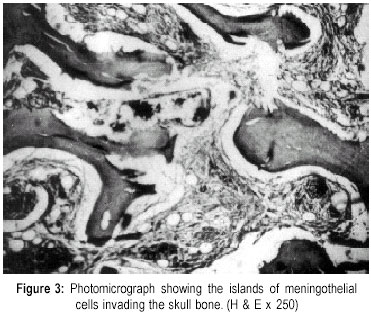
Calvaria, Orbit Case report A sixty-three year-old female complained of painful and progressive proptosis and chemosis of the left eye for six months. For 15 days she developed excessive lacrimation and diplopia. On examination, there was proptosis, the eyeball being displaced inferiorly. Vision, eye movements and rest of the neurological examination were normal. Skeletal survey was normal. Computerised tomography (CT) scan showed an en-plaque enhancing tumour extending over both frontoparietal convexity (Figure 1) and into the superolateral aspect of the left orbit displacing the eyeball inferiorly (Figure 2). The calvarial bone was thickened all along the length of the tumour. The patient underwent a left frontoparietal craniotomy. The bone was about 16-18 mm thick and was extensively vascular. The involved calvarium was resected widely. The extradural meningioma was diffuse and carpet like. It was soft and greyish and only moderately vascular. This mass was removed along with the involved markedly thick dura. The orbital roof and the orbital portion of the tumour were also removed. The dura was replaced with fascia lata dural graft. Bone defect created as a result of surgery was not reconstructed at this stage. Post-operative course was uneventful. Histological examination showed features of a meningothelial meningioma with the tumour consisting of sheets and whorls of meningothelial cells with vesicular nuclei. There was no mitotic activity or foci of necrosis (Figure 3). The patient was relieved of proptosis following surgery. However, she did not permit any further surgery for the right-sided tumour as well as for cranioplasty. Discussion Extracranial meningiomas are rare, the reported incidence being 1-2% of all meningiomas.(2) There are inconsistencies in nomenclature and inclusion criteria of meningiomas arising in locations outside the dural compartment.(1) They have been referred to as ectopic, extradural, calvarial, cutaneous, extraneuraxial or intraosseous meningiomas. To avoid this confusion, Lang et al has proposed a single term ‘primary extradural meningioma’ (PEM) for such lesions.(1) The dura and the dural sinuses are displaced away from the inner table of the skull in these cases. Bone remodelling and calvarial thickening is frequent with these tumours. Consequently, they are classified as purely extradural (Type I), purely calvarial (Type II) or calvarial with extradural extension (Type III). According to the site of location of the tumour they are further subdivided into convexity (C) or skull base (B) forms. Calvarial thickening at the site of origin of meningioma is common. The meningothelial cells invade into the calvarium and expand the bone. However, diffuse and widespread bone thickening is rare. Most of the similar cases reported were in the region of the frontal bone and involved the orbit and presented with the symptom of proptosis. En-plaque involvement of the dura is also associated with gliomatous, carcinomatous, sarcomatous and melanomatous invasion of the meninges. Many different hypotheses exist regarding the origin of primary extradural and calvarial meningioma. They are thought to arise from ectopic meningocytes or arachnoid cap cells trapped in the cranial sutures during moulding of the head at birth.(3) Misplacement and entrapment of meningothelial cells into suture or fracture lines as a result of trauma has also been speculated as the probable cause of calvarial meningioma.(4) Involvement of multiple sutures is also reported.(5) However, only 8% of the calvarial meningiomas are in relationship with a cranial suture. Cutaneous meningiomas could be congenital in origin where they can arise from arachnoid cell rests located in the skin as a result of defective closure of the neural tube wherein the meningeal tissue is ‘pinched’ off into the surface.(6) They are also thought to arise from multipotent mesenchymal cells as a reaction to an unidentified stimulus.(7) This may be relevant in our case since the meningioma was diffuse and involved the frontoparietal bone widely and extended into the overlying soft tissue. It had no special connection within the cranial sutures or the foramina of the cranial nerves. Calvarial meningiomas are known to be associated with intracranial hypertension.(5) The marked dural thickening overlying and adjacent to the tumour as well as the hyperostotic bone is attributed to cause intracranial hypertension. Dural sinus occlusion can also be an important cause of the raised intracranial tension. However, despite the extensive and diffuse frontoparietal hyperostosis, there was no evidence of raised intracranial tension in our case. Biologically, calvarial meningiomas have been observed to be benign and slow-growing. Calvarial meningiomas are more prone to develop malignant changes (11%) when compared to intracranial meningiomas (2%).(8) Meningiomas presenting with scalp swelling, osteolytic skull lesions and extracranial soft tissue masses are more aggressive in nature.(9) Computerized tomography with bone windows is helpful and MR imaging is useful in the evaluation of the extent of extradural and calvarial involvement. Angiography is non-specific and of little value. The differential diagnosis includes plasmacytoma, chondroma, chondrosarcoma, haemangioma, myeloma, eosinophilic granuloma, aneurysmal bone cyst, metastatic cancer or fipous dysplasia. Surgical resection is the treatment of choice. Although radiotherapy is advocated, it is usually not recommended unless there is evidence of rapid progression of the disease. In cases of diffuse involvement of the calvaria, a wide surgical resection is advisable whenever possible followed by a cranial reconstruction. The extracranial paraorbital spread of the meningiomas, although rare, is well known and the surgical strategies of such lesions have been well documented in literature.(10) If subtotal resection is performed due to the widespread extension or due to involvement of structures like the dura, orbit or paranasal sinuses, the lesion could be followed up at regular intervals with appropriate imaging studies. Fatal postoperative coagulopathy following excessive blood loss during surgery and massive blood transfusions are reported in large extracranial meningiomas.(10) Diffuse and extensive involvement of the dura, the skull and the orbit is a distinctive feature in our case and has not been recorded in literature. To conclude, bilateral and diffuse calvarial meningioma with extracranial extension is extremely rare. The en-plaque growth of the tumour, hyperostosis of the overlying calvaria, left orbital extension and alarming intraoperative haemorrhage can be a formidable surgical problem. Surgical extirpation is the treatment of choice. Radiation therapy is advocated for rapidly progressive disease. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01035f3.jpg] [jp01035f2.jpg] [jp01035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}