 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 47, Issue 2, 2001 pp.135-136 Ptuitary Metastases in Carcinoma Breast Rao SR, Rao RS Shushrusha Hospital, Shivaji Park, Mumbai - 400 028, India. Code Number: jp01040 A fifty-one-year-old postmenopausal
woman presented with a history of an ulcerated lump in the right breast of one-year
duration. It was 4 cm x 3 cm in size, in the central quadrant of the right breast.
There were no nodes palpable in the right axilla but she had a right supraclavicular
node. The left breast and left axilla were normal. Fine needle aspiration cytology
confirmed the lesion to be a carcinoma. Her baseline haematological and biochemical
investigations, X-ray chest, bone scan and ultrasound abdomen were normal. She
received two cycles of neo-adjuvant chemotherapy consisting of CMF regimen (cyclophosphamide,
methotrexate, 5-flourouracil). There was partial regression of the tumour. This
was followed by a right modified radical mastectomy. The histopathology report
was infiltrating duct carcinoma, with 11/11 axillary nodes positive for metastases.
Post-operatively, she was put on tamoxifen. She also received further four cycles
of chemotherapy (CMF) regimen and radiotherapy (RT) to the breast. She was asymptomatic
for two years following radiotherapy.
Two years later, she complained of excessive thirst, and generalised weakness.
She had a right-sided pleural effusion, which was confirmed to be malignant
on cytology. On admission in the hospital, it was found that her 24-hour urine
output was 4000cc. Her serum osmolarity was 253 mos/kg (normal 280-295 mos/kg),
and serum sodium, potassium and chloride levels were normal. Her serum antidiuretic
hormone level was 2.9 pg/ml, (normal 14 pg/ml). Urine osmolarity was 99 mos./kg
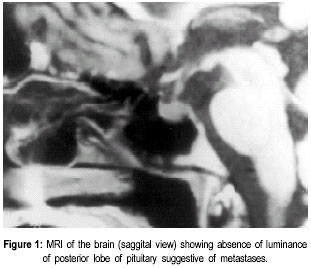
(normal 500-800 mos/kg). A magnetic resonance image (MRI) of the pain showed
absence of normal luminance of posterior pituitary, oedema and thickening of
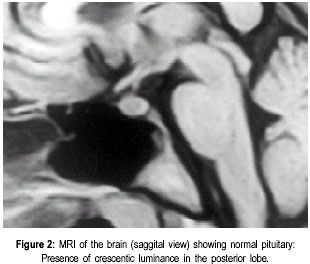
hypophyseal stalk (Figure 1). Posterior
pituitary is seen as a pight crescentic shadow in normal subjects (Figure
2). There were multiple small metastases in the brain. She was put on vasopressin by nasal insufflations and received radiotherapy. After radiotherapy her 24-hour urine output came down to normal levels and did not require vasopressin nasal insufflations. Discussion The incidence of metastasis to pituitary in breast cancer is reported as 0.95%.1 breast cancer and lung cancer are the most common primary sites, in women and men respectively, which metastasise to the pituitary.2 The presenting symptoms include diabetes insipidus, anterior pituitary insufficiency and retro-orbital pain. Metastases to the posterior lobe are more common than to the anterior lobe. The predilection of tumours to metastasise to posterior pituitary may be due to the fact that the neural portion has a blood supply directly from the systemic circulation while the anterior lobe is supplied by the hypothalamus-hypophyseal portal system.1 The clinical manifestation of such a metastasis is diabetes insipidus, which is often the presenting feature. De la Monte et al3 observed that patients who developed endocrine organ metastases were on an average of 5 to 10 years younger than those who had metastases to non-endocrine sites. They proposed that endocrine metastases occur in younger patients because the endocrine organs themselves provide a trophic influence for breast carcinoma cells, which require particular hormones for growth. However this may not be true in all cases. For example our patient was postmenopausal. A clinical diagnosis of diabetes insipidus is made in the presence of polyuria, polydypsia and in the absence of renal disease, diabetes mellitus, and psychogenic overhydration. Confirmatory tests are serum antidiuretic hormone levels, 24-hour urinary output, specific gravity of urine, plasma osmolarity and urine osmolarity.(4) All the above tests were suggestive of diabetes insipidus in our case. In the clinical context of a known cancer patient presenting with diabetes insipidus, MRI of the pituitary fossa is very useful in demonstrating metastases to the pituitary.(5,6) Loss of high signal from the posterior lobe and thickening of the stalk are indicative of infiltration by metastases.(7) The posterior pituitary is not a site that can be readily biopsied and hence the above findings on MRI in a known case of a cancer presenting with diabetes insipidus is taken as evidence of pituitary metastases. Satisfactory symptomatic relief from diabetes insipidus was achieved in most cases with vasopressin.(4) Efforts should be made to treat the underlying cause rather than mere symptomatic control of diabetes insipidus. Chemotherapy and radiation therapy have been used with variable degree of success. The median length of patient survival following diagnosis of pituitary metastases is 180-days.(2) Aggressive treatment including both surgical decompression and radiation therapy improves the quality of life in patients who are symptomatic. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01040f1.jpg] [jp01040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}