 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
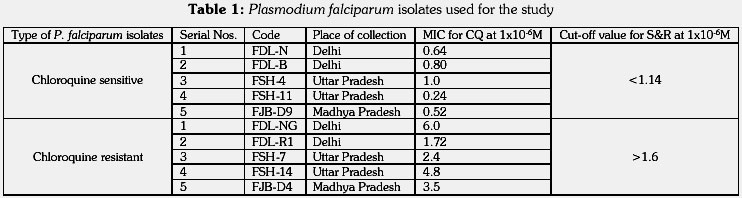
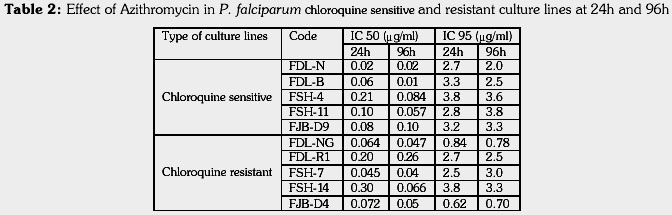
Journal of Postgraduate Medicine, Vol. 47, Issue 4, 2001 pp.240-243 In-vitro Antimalarial Activity of Azithromycin Against Chloroquine Sensitive and Chloroquine Resistant Plasmodium Falciparum Biswas SMalaria Research Centre (ICMR), 22 Sham Nath Marg, Delhi - 110 054, India. Code Number: jp01070 Abstract BAKGROUND: The spread of drug resistance in Plasmodium falciparum has made the situation essential to look into new effective therapeutic agents like antibiotics. Azithromycin is a potential, chemotherapeutic agent which possesses antimalarial activity and favourable pharmacokinetic properties. It is an azalide microbiocide derived semi-synthetically from macrolide erythromycin. Like other antibiotics, the azalide azithromycin has ability to inhibit protein synthesis on 70S ribosomes. SETTINGS: Experimental study. SUBJECTS AND METHODS: The parasiticidal profile was studied in five chloroquine sensitive and five chloroquine resistant P. falciparum isolates obtained from various places of India. The antimalarial activity was evaluated in P. falciparum schizont maturation by short term culture for 24 hours and by exposing the parasites to the drug for 96 hours. Parasites synchronized at ring stage were put for culture with various concentrations of azithromycin dihydrate (0.01-40mg/ml). RESULTS: At highest concentration (40mg/ml), parasite growth was inhibited totally in all 10 isolates. Antimalarial activity at 96 hours was greater than at 24 hours in both chloroquine sensitive and resistant parasites, which may indicate that the inhibition of parasite growth may occur at clinically achievable concentration of the drug when parasites were exposed for several asexual cycles. CONCLUSION: Azithromycin shows a potential for eventual use alone or in combination in the treatment of chloroquine sensitive and resistant P. falciparum malaria. Key Words: Malaria, P. falciparum, In-vitro culture, Drug sensitivity, Azithromycin Malaria has emerged as one of the major killer diseases in the world affecting 300 to 500 million people annually with nearly 1.5 to 2.7 million deaths due to malaria.(1) In India, 2.5 to 3 million malaria cases are recorded yearly as per the report of National Antimalaria Programme.(2) Of the four human plasmodia, the fatality has been observed in Plasmodium falciparum. This parasite has developed resistance to chloroquine and also to other antimalarial drugs.(3) Nearly 40% chloroquine resistant P. falciparum cases are recorded in India.(1) The spread of drug resistant P. falciparum has made the situation essential to look into new effective therapies like antibiotics. Antimicrobial agents like doxycycline, clindamycin, erythromycin, minocycline have been evaluated for their antimalarial activity but were found to have limited potential and more side effects. Fluoroquinolones have shown antimalarial activity both in vitro and in vivo.(4,5) Macrolide erythromycin and azalide azithromycin are essentially equipotent when tested as antimalarial; but an additive effect has been observed with azalide. Azithromycin has the potential to be an effective well-tolerated clinical prophylactic agent for P. falciparum malaria.(6,7) It is derived semi-synthetically from erythromycin and can inhibit protein synthesis by acting on 70S ribosomes.(8) It has predominant activity against erythrocytic stages of the parasite and also shows moderate activity against hepatic stages in experimental models and in human.(9,10) To start with a new product, it is always advisable to generate some data against the pathogens by various studies. Present in vitro study was planned in chloroquine sensitive and resistant strains of P. falciparum to evaluate antimalarial activity of azithromycin by exposing the parasites to short term and long-term cultures. Chloroquine as a known schizonticidal was taken as parallel control. Materials and Methods Azithromycin dihydrate (AZM) in the powdered form was obtained from Pfizer Ltd. A stock solution of 1mg/ml was prepared in 0.2ml ethanol (for dissolving) and 0.8ml sterile 0.015M phosphate buffered saline (PBS), pH 7.2. Wells of flat bottom microtitre tissue culture plates were dosed with 40, 10, 2, 0.5, 0.1, 0.02, and 0.01mg/ml concentrations of the drug. Wells with plain PBS were kept as control (without drug). The plates were dried under laminar flow, then sealed and stored until use. Chloroquine phosphate (CQ) in powdered form was obtained from SIGMA Chemical Company (St. Louis, USA). The microtitre plates were dosed with various 2-fold concentrations ranging from 1 to 64pmol/well as described elsewhere.(11) Indian P. falciparum isolates with variable sensitivity to CQ (in vivo and in vitro) were used in the study. Chloroquine sensitive and resistant strains were selected on the basis of patients’ response to CQ and in vitro susceptibility of clinical isolates to CQ. In pief the methodology was as follows: Patients reported in local/field clinic with fever were screened for malarial parasite. P. falciparum positive cases with asexual parasitaemia of above 1000 parasites/ml blood; with no history of taking CQ or other antimalarial drugs; with no history of intolerance to CQ were enrolled for in vivo and in vitro CQ sensitivity tests (day 0) after obtaining informed consent. An extended 28-day field test was used to monitor the therapeutic efficacy of CQ as per WHO guidelines and protocol(11-13). Enrolled patients were administered orally a total dose of CQ, 25mg/kg body weight over 3 days (10mg/kg on day 1 and day 2 followed by 5mg/kg on day 3). Thick and thin blood smears were examined for presence of asexual parasite (if any) on day 1, 2, 7, 14, 21 and 28 giving a total observation period of 4 weeks in each case. The in vitro test was performed on day 0 as per the published method(11). Blood samples from patients having P. falciparum ring stage at or above 1000 parasites/ml blood were collected aseptically in heparin before drug administration. Parasites were cultured at 5% haematocrit in 96-well flat bottom tissue culture plates pre-dosed with various concentration of CQ (1pmol - 64pmol) for 30 hours at 37oC by candle-jar technique.(14) Thick and thin smears were prepared from culture of each well. Schizonts having 8 or more nuclei were counted per 200 asexual parasites and the minimum inhibitory concentration was determined. Based on the CQ sensitivity status, five chloroquine sensitive (CQS) and resistant (CQR) strains of P. falciparum belonging to different geographic areas of India were taken for the study (Table 1). They were maintained in continuous culture by candle-jar technique(14). Parasites synchronized at ring stage were put for culture with AZM and CQ at 5% haematocrit with 0.5% parasitaemia. The antimalarial activity of AZM was evaluated by two in vitro assays: i) to determine the rate of schizont maturation by short term culture for 24h; ii) to determine whether the antimalarial activity of AZM could be enhanced by exposing the parasites for 2-cycles, i.e. 96h. Growth of the parasites from duplicate wells of each and every concentrations of the drug, was monitored microscopically by counting number of schizonts per 200 asexual parasites and total number of parasites per 5000 RBCs. Percent schizont maturation inhibition and total growth inhibition were calculated by the formula: (1-Nt/Nc)x100, where Nt and Nc represent the number of schizont/parasite in the test and control wells respectively. Inhibitory concentrations 50 and 95 were calculated in both CQS and CQR parasites by noting the drug concentrations at which 50% and 95% schizont maturation and total parasite growth were affected at 24h and at 96h. Results All 10 P. falciparum isolates did not grow at the highest concentration of AZM, i.e. at 40mg/ml, both in 24h and 96h culture. Parasite growth and reinvasion were significantly inhibited even at 0.1mg/ml. At 24h, trophozoites failed to mature to schizonts and there was a dose response effect of AZM on schizont maturation. However, at 96h overall effect of AZM in growth rate was observed, which may be due to the initial effect of AZM on schizont maturation. As observed in the present study the effect of AZM in both CQS and CQR parasites was almost similar. The mean IC50 and IC95 values are shown in Table-2. The IC50 values (mean + S.D.) for CQS and CQR parasites at 24h were 0.094 + 0.071 and 0.082 + 0.067; at 96h were 0.054 + 0.039 and 0.092+0.094 respectively. The IC95 values (mean + S.D.) for CQS and CQR parasites at 24h were 3.16 + 0.44 and 2.09 + 1.34; at 96h were 3.04 + 0.76 and 2.06 + 1.23 respectively. Discussion Findings of the study show that AZM inhibited the parasite growth more efficiently when the isolates were exposed for 96h (2-cycles), a substantial reduction in schizont maturation was also observed even at 24h. Minimum inhibitory concentration noted at 96h was 0.01mg/ml in CQS (FDL-B) and 0.04mg/ml in CQR (FSH-7). In earlier study, enhancement in antimalarial activity of AZM in P. falciparum was reported during one and two asexual erythrocytic cycles in established culture lines, K1 and FC(15). The MICs after 48h of incubation was 6.2 and 8.7mg/ml, whereas after 96h they were 0.08 and 0.04mg/ml in K1 and FC lines respectively. In present study, pronounced antimalarial activity has been observed after 24h, but no further reduction in the MIC was noted during 96h exposure. This might be due to the assay conditions followed in this study. Parasites were exposed to drug for 96h without changing of media and addition of drug, therefore, parasite population survived, though less in number, remained there either viable or unviable. Besides the antimalarial activity, AZM has been used as an effective agent for Cryptosporidiosis in experimental animals(16) and an effective alternative for the treatment of Campylobacter enteritis in travelers(17). Its in vitro activity has also been observed in clinical isolates of Neisseria gonorrhoeae (presented in seminar). The efficacy of AZM in human P. falciparum malaria has been reported(9). Effect of AZM on malariometric indices in Gambia has been shown during a randomized study in children of 5-14 year age group. The effect was related more to resolution of parasitaemia than to prevention of new infections(18). In a recent study, effect of AZM on nucleoside-5’ triphosphates (NTPs) and 2’- deoxynucleoside-5’ triphosphates (dNTPs) levels were compared in P. falciparum and human leukaemia cells. The drug caused more severe effects on the levels of NTPs and dNTPs in P. falciparum compared to leukaemia cells, which may provide an explanation for selective activity against malaria and its utility as antimalarial drug(19). With a view to look for alternative drugs for the treatment of multidrug resistant falciparum malaria, further studies are to be undertaken to determine the antimalarial properties of AZM in human malaria model. Such studies are relevant because AZM is an effective antibiotic and the results of such studies carry immense values. The practical value of AZM as an antimalarial drug would bear high significance if the clinical studies indicate that it can combat malaria infection alone. This drug could also be very useful in combination with a rapidly acting but non-curative antimalarial in case of treating drug resistant malaria. Azithromycin may prove to be a promising new antimalarial agent in drug resistant P. falciparum infection which causes cerepal malaria and is responsible for maximum morbidity and mortality in various states of India. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01070t1.jpg] [jp01070t2.jpg] |
| |||||||||

{kind=link}
{kind=link}