 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
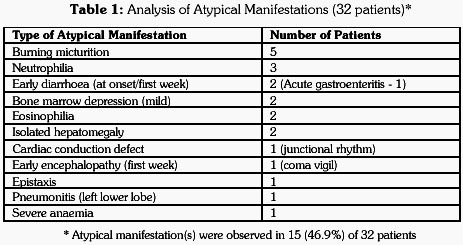
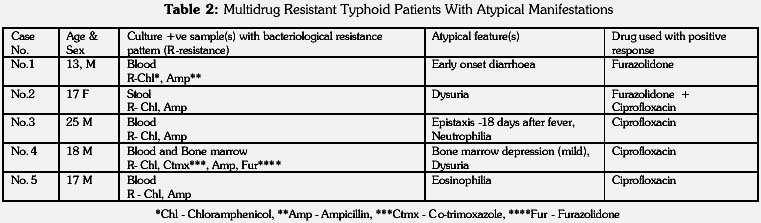
Journal of Postgraduate Medicine, Vol. 47, Issue 4, 2001 pp. 248-251 Atypical Manifestations of Typhoid Fever Dutta TK, Beeresha, Ghotekar LHDepartment of Medicine, JIPMER, Pondicherry – 605 006, India Code Number: jp01072 Abstract BACKGROUND: High fever, toxaemia, constipation during first week of fever, complicated by encephalopathy and perforation during third week of fever are the typical manifestations of typhoid fever. However, the classical presentation of typhoid fever has considerably changed now. AIM: To study atypical presentations of typhoid fever. SETTING: A teaching unit of a hospital in South India METHOD: All culture-positive adult patients of typhoid fever admitted over a period of seven years were studied RESULTS: Thirty-two adult patients were admitted. Fifteen (46.9%) patients presented with atypical manifestations. Atypical manifestations observed were burning micturition with normal urine examination (n= 5, 15.6%) diarrhoea in first week (6.2%), encephalopathy in first week (3.1%), isolated hepatomegaly (6.2%), pneumonitis (3.1%) and bone marrow depression (6.2%). Out of 32 Salmonella typhi culture positive patients, 10 (31.3%) patients had multidrug resistant (MDR) strain. Patients with MDR strains had atypical manifestations (5/10=50%) not significantly more often than patients having multidrug sensitive strains (10/22=45.5%) (Z <2). All patients responded to treatment. CONCLUSION: It appears atypical manifestations do not necessarily mean a worse prognosis in typhoid fever. Patients having high fever presenting with pneumonia, early encephalopathy, early diarrhoea or bone marrow depression in a typhoid endemic area, should be suspected for this disease. Key Words: Pneumonitis, Early encephalopathy, Early diarrhoea, Bone marrow depression. High fever, toxaemia, constipation during first week of fever, diarrhoea during second week of fever, mild splenomegaly and leucopenia/neutropenia, complicated by encephalopathy, intestinal haemorrhage and perforation during third week of fever are the typical manifestations of typhoid fever.(1)However, with more and more information being available, features not very characteristic of typhoid fever are being more often attributed to typhoid fever. The features described vary from psoas pyomyositis(2) to splenic abscess,(3) splenic rupture(4) and liver abscess(5) at one end of spectrum to cerebellar ataxia,(6) schizophrenia(7) and suicide(8) at other end of spectrum. Factors responsible may be from multidrug resistance shown by Salmonella typhi to incomplete treatment with common antibiotics. Our aim in this study was to analyse the atypical manifestations of typhoid fever as observed in adult population. Subjects and MethodsData of all adult patients of culture-positive typhoid fever admitted over a period of seven years in one unit of a teaching hospital in South India were analysed for atypical manifestations. For the purpose of analysis, patients were divided into early and late entry groups according to their hospital entry before and after three weeks of developing fever - to see if there was any variation in their presentation. Besides looking for typical manifestations like high fever (temperature >101 F [38.3 C]),(9) vomiting, constipation during first week and diarrhoea during second week, splenomegaly etc., each patient’s record was verified for occurrence of any atypical manifestation during the illness. Results Thirty-two (age >13 years, 19 males and 13 females) culture-positive typhoid fever patients were admitted during the period. The mean age of the patients was 23.9 years (range 13-55 years); one patient was aged 55 years. Twenty-six patients entered the hospital before three weeks of fever. They belonged to early entry group. Six patients entered after three weeks of fever. Salmonella typhi was isolated from cultures of blood, bone marrow or stool (Blood – 27, stool – 1, blood and bone marrow – 1, blood and stool – 1, blood, bone marrow and stool – 2). 15 (46.9 %) of 32 patients had atypical manifestations. Thirteen of them belonged to early entry group and two to late entry group. Atypical manifestations observed are enlisted in Table 1. Pneumonitis was observed in one (3.1%) patient (Table 1). This 25-year-old female patient with left lower lobe pneumonitis came after 12 days of fever. No other cause for pneumonia could be found. Blood culture grew Salmonella typhi and patient recovered completely after a course of ciprofloxacin. Burning micturition was observed in 5 (15.6%) patients. Urinary examination, however, revealed no abnormality and the symptom resolved with treatment of typhoid fever. Early diarrhoea i.e., diarrhoea as a presenting feature or diarrhoea during first week of illness, was observed in two (6.2%) patients; the mean age of these patients was 17 years. One patient had acute gastroenteritis at onset. Other atypical gastrointestinal symptom observed was isolated hepatomegaly. Isolated hepatomegaly was observed in two (6.2%) patients; however, none of the patients had jaundice. Hepatomegaly was mild in one and moderate in another case and it resolved with treatment of typhoid fever. Early encephalopathy i.e., encephalopathy during the first week of illness, was one of the grave complications observed in one (3.1%) of our patients. A 17-year-old female developed altered sensorium followed by coma vigil on third day of fever. Patient, however, responded to treatment with ciprofloxacin. One patient presented with epistaxis on 18(th) day of fever. Blood culture grew Salmonella typhi, sensitive to ciprofloxacin and resistant to cotrimoxazole and chloramphenicol. One 13-year-old male presented with cardiac manifestation in the form of transient junctional rhythm. The electrocardiographic abnormality resolved spontaneously with treatment of typhoid fever. Neutrophilia was observed in three (9.4%) patients. One (3.1%) patient had severe anaemia with Hb of 5g/dl without any apparent cause. Two (6.2%) patients had eosinophilia. Two (6.2%) patients had developed bone marrow depression. One patient admitted after two weeks of fever, had mildly hypocellular marrow and the patient responded to cotrimoxazole and furazolidone. Second patient admitted after three weeks of fever had mild bone marrow depression. This patient responded to treatment with ciprofloxacin. None of the patients who developed bone marrow depression had received chloramphenicol, nor any other cause for bone marrow depression was found in them. Nine patients presented with a single atypical manifestation; six patients presented with multiple atypical manifestations. Incidence of atypical presentation in early (13/26 = 50%) and late (2/6 = 33.3%) entry group did not correlate with duration of illness. However, multiple atypical presentations were seen more often in late entry group (2/6 = 33.3%) as compared to in early entry group (4/26 = 15.4%). Out of 32 Salmonella typhi culture positive patients, 10 (31.3%) patients were multidrug resistant. Bacteria was considered to be multidrug resistant, if found resistant to chloramphenicol, ampicillin and/or co-trimoxazole.10,11 Antibiotic sensitivity was tested for chloramphenicol, ampicillin, cotrimoxazole, cefotaxime, ciprofloxacin, furazolidone and gentamicin. Patients with multidrug resistant (MDR) strains had atypical manifestations (5/10=50%) not significantly more often than patients having multidrug sensitive strains (10/22=45.5%) (Z <2). Profile of five, out of ten patients with MDR typhoid, who presented with atypical manifestations, is given in Table 2. The various drugs used amongst the patients in order of frequency were ciprofloxacin, furazolidone, pefloxacin, gentamicin, cotrimoxazole, chloramphenicol, cefotaxime, ampicillin and amoxycillin. All patients responded to treatment. Atypical manifestations in all patients resolved with treatment of primary condition, i.e., typhoid fever. All the 10 patients with MDR typhoid fever also responded to treatment. Majority of them received ciprofloxacin. Discussion The classical picture of typhoid fever has changed over the years. Atypical presentation seen more often than not nowadays may delay the clinical suspicion of the disease. All patients who visit hospital in an endemic area come after receiving some treatment. This presumably has altered the presentation of the disease significantly. One (3.1%) of our patients presented with pneumonitis. This patient had come to us after 12 days of fever and belonged to early entry group. This was significant, since this atypical presentation could not be attributed to delay in instituting treatment. During the phase of sustained (secondary) bacteraemia, which coincides with the first week of fever, very few organs escape invasion by bacteria,(11) and this probably is the cause of several atypical manifestations seen even during the early phase of disease. Early diarrhoea as presenting symptom is well known in children. We had two adult patients who presented with diarrhoea during the first week and one of them presented with acute gastroenteritis at the onset itself. It appears occasionally adolescents and young adults can also present with diarrhoea (or even acute gastroenteritis). Isolated hepatomegaly is uncommon in typhoid fever except perhaps in multidrug resistant typhoid fever.(12) We noticed it in two patients who did not have multidrug resistance. Encephalopathy or typhoid state is a well-recognised entity in typhoid fever.(11) This occurs typically in third week of illness.(11) Early encephalopathy (i.e., during first week), as observed in one of our patients is uncommon. It must be considered as a grave sign; nevertheless, our patient improved. We observed epistaxis on 18th day in one case. The possible mechanism could have been vasculitis. Bone marrow depression was observed in two of our cases. In a carefully conducted prospective study elsewhere, some form of bone marrow suppression was observed in 16 (44.5%) of 36 patients of typhoid fever.(9) We found incidence of atypical manifestations with almost equal frequency in early and late entry groups and almost every other patient had some atypical manifestation. However, these atypical manifestations did not necessarily mean a poor prognosis. The gold standard of treatment for enteric fever now, amongst other drugs, is a 4-fluoroquinolone or a third generation cephalosporin, especially in multidrug resistant states.(10,11,13) Elsewhere, MDR typhoid fever has been described to be associated with graver prognosis and three-fold increase in mortality.(12) However, all of our MDR patients responded to treatment. Our case-fatality rate was zero percent. The general observation is that case-fatality rate rarely exceeds 1% if promptly treated.(14) To conclude, “atypical” presentations are seen quite often now. Despite the high number of unusual presentations and the late date of presentation in some cases, outcome is quite good. We feel this report represents the norm in endemic areas now. Our findings have some important ramifications. Physicians caring for patients in India and elsewhere in endemic areas should certainly suspect typhoid fever in patients who present atypically with pneumonia, gastroenteritis, early encephalopathy, etc. References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2001 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp01072t1.jpg] [jp01072t2.jpg] |
| |||||||||

{kind=link}
{kind=link}