 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 1, 2002 pp. 29-31 Primary Pleuro-pulmonary Malignant Germ Cell Tumours Vaideeswar P, Deshpande JR, Jambhekar NA* Departments of Pathology, Seth G. S. Medical College and *Tata Memorial Hospital,
Mumbai - 400 012, India. Code Number: jp02008 Abstract: Lungs and pleura are rare sites for malignant germ-cell tumours. Two cases, pure yolk-sac tumour and yolk sac-sac tumour/embryonal carcinoma are described in young males who presented with rapid progression of respiratory symptoms. The malignant mixed germ cell tumour occurred in the right lung, while the yolk-sac tumour had a pseudomesotheliomatous growth pattern suggesting a pleural origin. Alpha-foetoprotein was immunohistochemically demonstrated in both. Key Words: Germ cell tumours, Extragonadal, Malignant, Pleura,Lung Extragonadal germ cell tumours are rare lesions and are mainly located in the retroperitoneal, mediastinal, pineal and presacral regions.1,2 Lungs and pleura are extremely uncommon sites for such tumours. We report two cases of malignant germ cell tumours in young males.
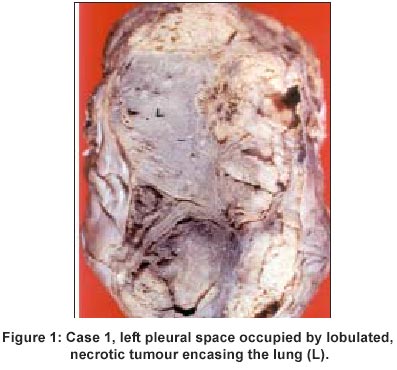
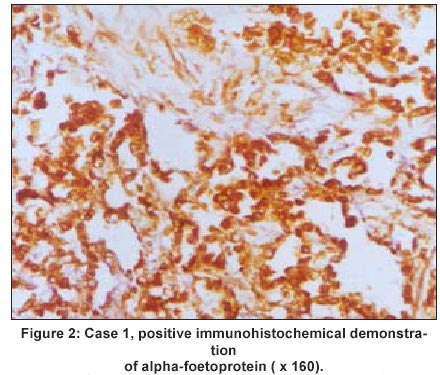
Case History Case 1 A 14-year-old male presented with low-grade fever, cough with mucoid expectoration and progressive breathlessness for the 15 days. On examination, the boy was febrile with tachycardia and respiratory distress. The trachea was shifted to the right with left-sided dull percussion note and decreased vocal resonance. The clinical impression was of left pleural effusion with collapse of the left lung, probably tuberculosis. Chest radiography revealed diffuse opacification of the left side. Undifferentiated small round cells were seen on fine-needle aspiration cytology. However, the child died before further investigations could be carried out. A complete autopsy was performed. The heart weighed 60 gm. and was normal. The whole of the left pleural cavity was occupied by a highly mucoid, lobulated, soft, necrotic grey white mass completely encasing the left lung in a mesotheliomatous pattern (Figure 1). Apart from collapse, the left lung parenchyma was normal. There was no intrabronchial or parenchymal tumour. The right lung was normal. No tumour was seen in the testes, retroperitoneum, mediastinum and other organs. The tumour, on histology, showed features of a yolk-sac tumour with microcystic and papillary patterns. The tumour cells had moderate amounts of pink cytoplasm and mildly pleomorphic nuclei with coarsely clumped chromatin. The intervening stroma was loose and myxoid. Intracytoplasmic and extra cellular PAS-positive, diastase resistant hyaline droplets were frequently seen. Immunohistochemistry for alpha-foetoprotein was strongly positive (Figure 2). No other germ cell elements were identified in the tumour or in any other organ, including the testes. Hence a diagnosis of primary pleural yolk-sac tumour was made.
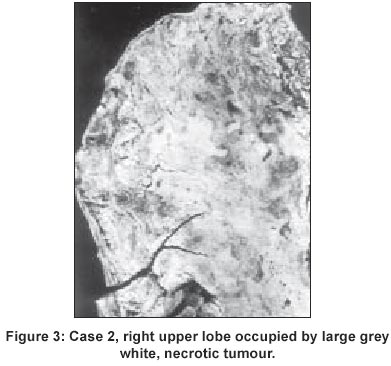
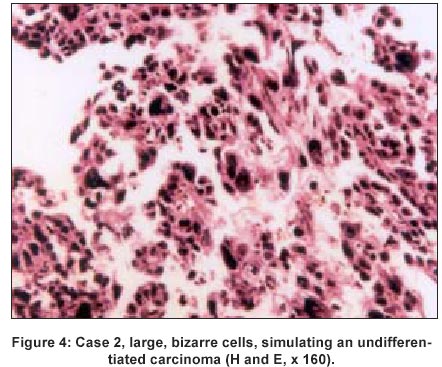
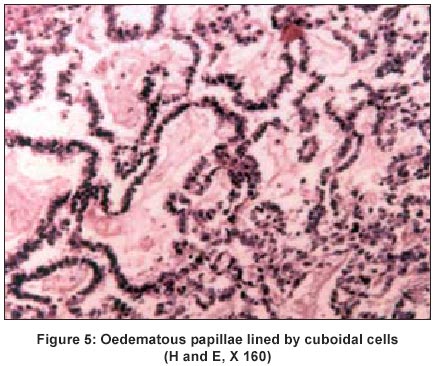
Case 2 A 20 year-old-male had a rapidly progressive dyspnoea with associated fever, cough, chest pain, anorexia and weight-loss for the past one month. The clinical impression was tuberculosis. The haematological and biochemical parameters were within normal limits. Computed tomographic scan of the chest revealed a well-defined, heterogeneous mass in the upper zone of the right lung with minimal right pleural and pericardial effusions. The patient expired within two days of admission. At autopsy, the right and middle lobes were voluminous and wholly occupied by a large (13x12x12 cm), well circumscribed, tan-coloured necrotic tumour (Figure 3). The pleura overlying the tumour was markedly thickened, opacified and adherent to the parietal pericardium. In addition, there were two smaller nodules, grey white to light brown in colour, in the anterior and posterior basal segments of the right lower lobe. The right hilar and carinal lymph nodes were enlarged, grey white and necrotic. Multiple sections from the tumour and lymph nodes showed necroses and haemorrhage with a peripheral rim of viable tumour cells. The cells were largely in sheets with moderate to abundant eosinophilic to clear cytoplasm and extremely pleomorphic nuclei. Bizarre forms and giant cells were scattered throughout (Figure 4). However, in some areas, the cells showed papillary and glandular pattern with loose textured stroma (Figure 5). The cells were found to be focally positive for cytokeratin and strongly positive for alpha-foetoprotein;human chorionic gonadotrophin (HCG), and placental alkaline phosphatase were negative. The impression was of an embryonal carcinoma with yolk-sac tumour of the lung. Primary germ cell tumour elsewhere was ruled out. The left lung had multiple fresh haemorrhagic infarcts due to occlusive pulmonary arterial thrombi. The cause of death was attributed to acute thrombosis of the dominant right coronary artery and acute myocardial infarction.
Discussion A diagnosis of a malignant extragonadal germ cell tumour can be established if the criteria laid by Einhorn3 are fulfilled. They include absence of a detectable (including stigmata of burnt-out lesion) or subsequent appearance of a gonadal tumour and absence of nodal metastases in the para-aortic and iliac regions. With these stringent criteria, the lung emerges as an extremely uncommon site for such tumours. Most of them have been mixed germ-cell tumours. In an early study by Holt et al,4 20 teratomatous tumours were found to involve the thoracic region. Seven among these were excluded because of probable mediastinal location. Thirteen had primary pulmonary location and five of these were malignant. In a recent review by Miller et al5 and Pont et al,6 30 cases of germ cell tumours and about 12 cases of malignant tumours, respectively, were reported. Histologically, these tumours have been teratoma with embryonal carcinoma and yolk-sac tumour components4,5,7,8 or teratomas with malignant transformation4 or embryonal carcinoma mixed with yolk-sac tumour2 or seminoma.6,9 Inoue and associates have reported pure yolk-sac tumour of the lung once.10 In the present report, one was a pure yolk-sac tumour while the other was combined with embryonal carcinoma. There is a general agreement that these tumours occur in the younger age group, grow rapidly, are large and necrotic and associated with elevated levels of alpha-foetoprotein and HCG. All the cases were located within the lungs as was seen in case 2. However, a pleural yolk-sac tumour encasing the lung in a mesotheliomatous pattern with compression of the lung has never been reported. Both the cases were strongly positive for alpha-foetoprotein immunohistochemically, Serum levels were not estimated, as a clinical diagnosis of germ cell tumour was not entertained. In fact, Richardson and group designated such tumours as "unrecognised extragonadal germ cell cancer syndrome."11 They studied 12 patients diagnosed as poorly differentiated or large cell undifferentiated carcinomas. Lung was involved in six patients;isolated lung involvement was not present. There was no detailed pathologic description. Recognising such lung tumours in patients is important because these tumours are sensitive to chemotherapy with increased patient survival. At the same time, such tumours should not be over-diagnosed especially in the elderly since non-germ cell epithelial malignancies can also produce alpha-foetoprotein.2,12
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02008f5.jpg] [jp02008f1.jpg] [jp02008f3.jpg] [jp02008f2.jpg] [jp02008f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}