 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 2, 2002 pp. 119-121 Cavernous Sinus Syndrome as the Only Manifestation of Sarcoidosis Zarei M, Anderson JR,* Higgins JN,** Manford MR Departments of Clinical Neurology, Neuropathology* and Neuroradiology,** Addenbrooke's
Hospital, Cambridge University, Hills Road, Cambridge CB2 2QQ, UK. Code Number: jp02038 Abstract: We describe a 63-year-old Afro-Caribbean female who presented with complete ophthalmoplegia of the right eye. Magnetic resonance imaging revealed a mass in the cavernous sinus, which was pathologically confirmed as due to sarcoidosis. No clinical or laboratory evidence of sarcoidosis was found in any other organs. We believe this is the first reported case of an isolated cavernous sinus syndrome due to sarcoidosis and suggest that sarcoidosis should be considered in the differential diagnosis of cavernous sinus syndromes even in the absence of systemic involvement of sarcoidosis. Key Words: Sarcoidosis, cavernous sinus, ophthalmoplegia. Sarcoidosis, a systemic non-caseating granulomatous disease, was first distinguished as a skin lesion by Hutchinson in 1875.1 Winkler described involvement of central nervous system (CNS) in 1905.1 Jefferson also distinguished three syndromes associated with involvement of cavernous sinus by sarcoidosis according to the location of the pathology.1 The anterior syndrome comprised deficits of the ophthalmic branch of the trigeminal nerve, and all the nerves innervating ocular muscles. The middle syndrome included the first and second branches of the trigeminal nerve, with denervation of varying ocular muscles and the posterior syndrome involved the oculomotor and abducens nerves and the entire trigeminal nerve, including its motor component. Since then several cases of sarcoidosis of cavernous sinus have been described,2,3,4,6 but all of these were in the context of systemic involvement. We believe this is the first reported case of an isolated cavernous sinus syndrome due to sarcoidosis.
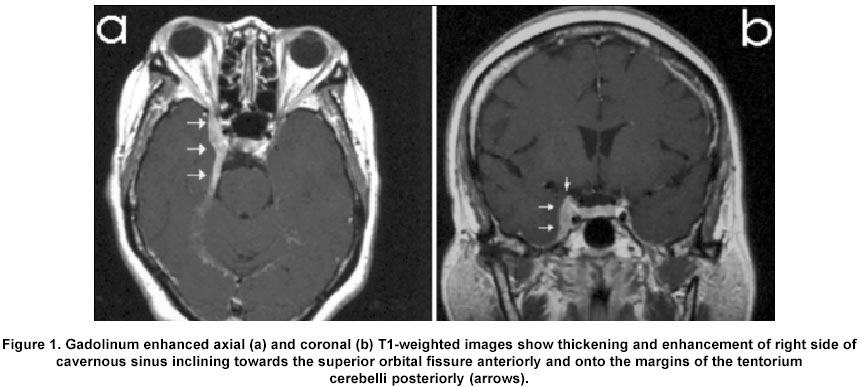
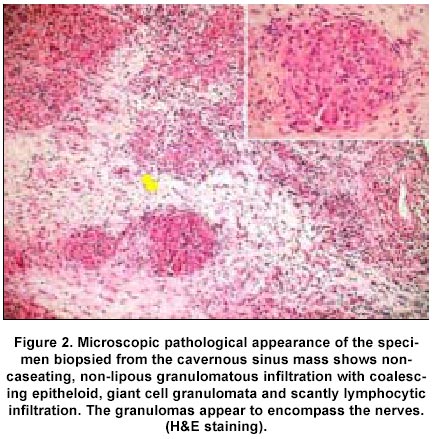
Case History A 63-year-old Africo-Carribean woman presented with a one-week history of pain in the right retro-orbital region associated with right-sided facial paraesthesia. Over the next few days, before she presented, she developed diplopia and right-sided ptosis. She had no systemic symptoms but had a complex medical history including adult onset insulin-dependent diabetes mellitus, asthma, essential hypertension, hyperchol-estrolaemia, sickle cell trait, deep vein thrombosis, lymphoedema, carcinoma of the cervix treated with total hysterectomy 30 years earlier, oesophageal stricture and functional dysphonia. She did not smoke. Her medication was nifedipine slow release 40mg twice daily; Simvastatin 10 mg nocte; Human Mixtard 14 IU twice daily; Bendrofluazide 5 mg daily and Codydramol two tablets four times daily. Her personal, social and family history were otherwise unremarkable. On examination she was overweight but general physical examination was otherwise unremarkable. Neurological deficits were confined to the right eye where there was mild periorbital oedema, slight proptosis and complete palsies of oculomotor, trochlear, and abducens nerves. The right pupil was fixed and dilated. Visual acuity was 6/18 in both eyes with spectacles and visual fields were full. There was a slight reduction of sensation in ophthalmic and maxillary branches of trigeminal nerve. The right corneal response was impaired, consistent with right trigeminal abnormality. The following investigations were normal or negative: complete blood count, blood urea, serum electrolytes, liver function, thyroid function, immunoglobulin electrophoresis, serum angiotensin converting enzyme (ACE), prothrombin time, partial thromboplastin time, autoimmune profile including anti-neutrophil cytoplasmic antibodies, cardiolipin and phospholipid antibodies, chest x-ray, lung function tests, gallium scan and computerised tomographic brain scan. Magnetic resonance imaging (MRI) scan with Gadolinium showed retro-orbital and meningeal enhancement particularly in the area of cavernous sinus (Figure 1). Erythrocyte sedimentation rate was elevated at 57 mm at one hour. Cerebrospinal fluid (CSF) cell count was normal but the protein was slightly elevated at 0.64 gm/d L and there were similar oligoclonal bands in CSF and in blood pointing to a systemic disorder with CNS involvement rather than a purely CNS disorder. The cavernous sinus lesion was biopsied under direct vision. Peroperatively the mass appeared confined to the cavernous sinus. Histopathological examination showed granulomas with multinucleated giant cells but no caseation or lipidification and no evidence of mycobacteria or fungi (Figure 2). We made a diagnosis of sarcoidosis. She received intravenous methylprednisolone, 1 gram daily, for 3 days then oral prednisolone 60 mg daily. Her eye movements improved over 2 weeks and the dose of prednisolone was tapered rapidly to 20mg daily over the next 4 weeks because of the development of mild steroid-induced confusion. By this time full eye movements and pupillary responses had returned but a moderate partial ptosis persisted.
Discussion Cavernous sinus syndrome is characterised by involvement of the cranial nerves passing through the sinus: oculomotor; trochlear; abducens and the ophthalmic and maxillary divisions of the trigeminal nerve. Causes of cavernous sinus synd-rome include thrombosis, tumours (e.g. meningioma and lymphomas), infective masses such as mycetomas (e.g. tuberculosis and mucormycosis) and inflammatory masses (e.g. sarcoidosis and Toloso-Hunt syndrome). Considering the clinical presentation and laboratory findings the closest differential diagnoses were sarcoidosis and Tolosa-Hunt syndrome. In this case characteristic granulomatous changes with giant cell formation was typical of sarcoidosis. Giant cells are rarely found in histopathology of Tolosa-Hunt syndrome in a background of lipogranulo-matous changes.5 In addition, usually in Tolosa-Hunt syndrome abnormal blood cell counts, positive ANA and increased serum globulins are also found5 and MRI scan usually show variable enhancement associated with involvement of orbital muscles.7 Involvement of the CNS in systemic sarcoidosis is well described in 5-10% of cases but is uncommon as the first manifestation of the disease. Cavernous sinus involvement usually occurs in the context of more widespread CNS disease; we believe this is the first report of primary cavernous sinus sarcoidosis with no apparent involvement elsewhere. Previously, one case of posterior cavernous sinus syndrome was reported following localised pachymeningitis with sarcoidosis,2 however there were systemic involvement characterised by lymphadenopathy and fever. The clinical and MRI findings may easily mislead the clinician to the diagnosis of retro-orbital pseudotumor or meningioma. Nafat and colleagues6 also described such a case with past history of systemic sarcoidosis. The present case shows sarcoidosis can primarily involve cavernous sinus and should be considered in differential diagnosis of cavernous sinus syndrome either thrombosis or mass. Common laboratory tests including CSF and serum ACE are rarely helpful in the diagnosis of isolated neuro-sarcoidosis. Neuroimaging especially MRI scan with and without gadolinium is the most useful non-invasive test. Meningeal enhancement is a common but non-specific finding in intracranial sarcoidosis, occurring also in chronic infectious and neoplastic meningitis. Diagnosis rests with histopathological examination. We were especially keen to exclude mucormycosis fungal infection of the cavernous sinus, a rare but recognised and very dangerous complication of diabetes mellitus, for which corticosteroids would have been contraindicated.
Acknowledgment Authors are grateful to Mr. Rodney Laing and Dr. Sidharthan Chandran for their collaboration in patient care and investigation.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02038f1.jpg] [jp02038f2.jpg] |
| |||||||||

{kind=link}
{kind=link}