 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 2, 2002 pp. 127-128 Coexisting Chondroblastoma and Osteochondroma: A Case Report Pardiwala D, Agarwal M, Puri A, Vyas S Bone and Soft Tissue Service, Department of Surgery, Tata Memorial Hospital,
Parel, Mumbai - 400 012, India. Code Number: jp02041 Abstract: The coexistence of two different types of benign cartilaginous tumours of bone in the same patient has not been reported in literature. We report a case in which a sixteen-year-old male had a benign chondroblastoma of the proximal left humerus and an osteochondroma of the distal left femur. Both originated at the same time and had a progressive increase in size with growth. Key Words: Osteochondroma, chondroblastoma, chondral tumours, cartilage germ cells. Benign chondromatous tumours of bone include a rather diverse group of lesions arising both from within bones (enostotic) and from the surface of bones (exostotic). In conditions like Diaphyseal Aclasis (osteochondromatosis) and Ollier's Disease (enchondromatosis), similar cartilage tumours arise at multiple sites. Though some theories have been put forth explaining common pathogenic factors, to the best of our knowledge, the coexistence of two different types of benign cartilaginous tumours of bone in the same patient has not been reported in literature. We report a case in which a sixteen-year-old male had a benign chondroblastoma of the proximal left humerus and an osteochondroma of the distal left femur. Both originated at the same time and had a progressive increase in size with growth.
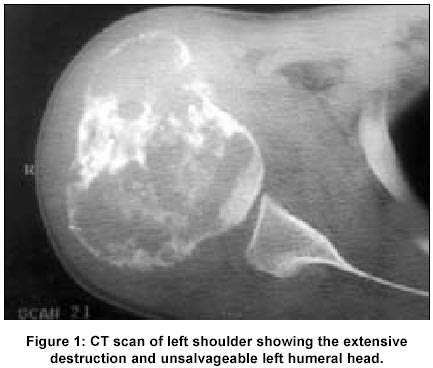
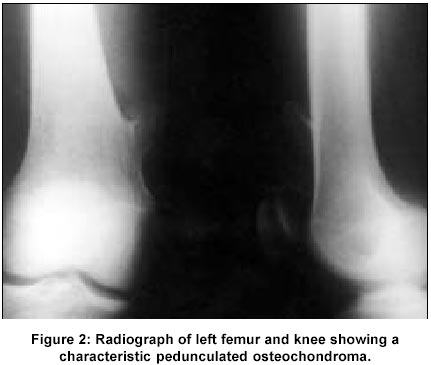
Case History A sixteen year old male presented with complaints of two swellings over his body; one in the region of his left shoulder, and another just proximal to his left knee on the medial aspect. Both swellings were first noticed at thirteen years of age and had gradually progressed in size over the past three years. Although the shoulder swelling had been painful for over a year now and had caused significant loss of shoulder function, the swelling proximal to his left knee had become painful following trivial local trauma a month prior to presentation. A radiograph of the left shoulder revealed an osteolytic lesion of the proximal epi-metaphyseal region of the humerus with a sclerotic border and narrow zone of transition. Located centrically, it demonstrated punctate calcifications and a periosteal reaction. The superior part of the humeral head showed large cortical discontinuity with destruction of a portion of articular surface. A CT scan of the region (Figure 1) besides delineating the extent of destruction, revealed cortical discontinuity and a soft tissue component with heterogeneous enhancement around the peripheral aspect of the large tumour. A radiograph of the left knee and femur (Figure 2) revealed a classical pedunculated exostosis arising from the medial aspect of the distal femoral metaphysis. A Needle biopsy of the proximal humeral swelling revealed a benign chondroblastoma showing occasional multinucleate giant cells. The femoral exostosis was not subjected to a preoperative biopsy. The patient underwent a wide excision of the proximal end of humerus with a live vascular fibula transfer. The fibular head was arthrodesed with the glenoid and the entire construct was fixed with a long 4.5 mm. narrow plate. The femoral exostosis underwent a marginal extracapsular resection that included the entire cartilagenous cap and overlying perichondrium and periosteum. Histopathological examination of the tissues confirmed a benign chondroblastoma of the proximal humerus and an osteochondroma of the distal femur. The chondroblastoma demonstrated peripheral cortical destruction with soft tissue extension and fifty percent destruction of the humeral articular surface. The patient made an unremarkable recovery and has satisfactory function of his shoulder arthrodesis with no recurrence of either tumour at a two year follow-up.
Discussion The differential diagnosis for coexisting multiple tumours is: skeletal malformations like diaphysial aclasis, or Olliers disease where multiple similar tumours are present throughout the skeleton; malignancy developing in one of the multiple tumours like in multiple exostoses or neurofibromatosis; metastasis from a primary malignant tumour; multifocal tumours such as occasionally in giant cell tumour or osteosarcoma; giant cell tumour developing in an aneurysmal bone cyst; and bery rarely two different tumours. Osteochondroma and chondroblastoma are similar neoplasms in that both are benign chondral tumours of bone, the cells of which exhibit a staining reaction for S-100 protein.1 Although tubulin is detected in both chondroblastomas and osteochondromas, tau expression is absent in both these tumors.2 There are theories related to anatomic considerations and pathogenesis. The physeal plate has been implicated in the aetiology of both tumours and they are believed to derive from displaced cartilage germ cells.3,4 The locally aggressive variety of benign chondroblastoma (as shown in this case report) is well documented in literature.5,6,7 We however could not find a single case in which two benign cartilage tumours of bone coexisted in the same patient. This is interesting considering that both neoplasms having a common pathogenetic origin (from the physeal plate) progressed to two different pathological entities at two different sites in the same patient.
References
This article is also available in full-text from http://www.jpgmonline.com/
© Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02041f2.jpg] [jp02041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}