 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 2, 2002 pp. 133-134 Foetus in Fetu Nagar A, Raut AA, Narlawar RS Department of Radiology, Seth G. S. Medical College and K. E. M. Hospital,
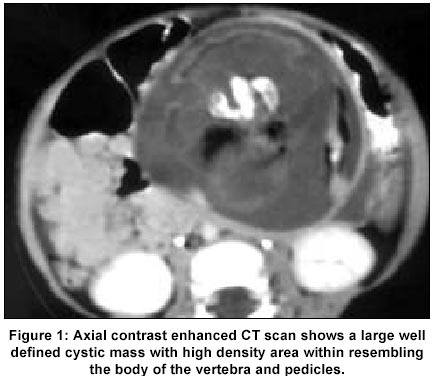
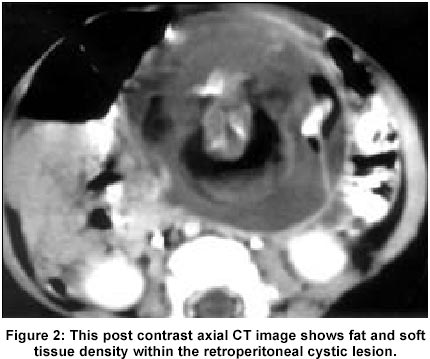
Parel, Mumbai - 400 012, India. Code Number: jp02044 A 2-year-old boy presented with gradual distension of the abdomen with an abdominal lump and 2-3 episodes of vomiting. There was history of low-grade intermittent fever. On examination the swelling was firm, ill-defined, globular, non-tender and moved with the respiration. Plain radiograph of the abdomen revealed a well defined mass of approximately 6 cm X 5 cm size, with a definite irregular hyperdense lesion in the right hypochondrium, displacing the bowel loops and the stomach. Ultrasonography (USG) of the abdomen showed a mixed echogenic predominantly cystic areas with large calcific foci causing posterior shadowing. Plain and contrast enhanced computed tomography (CT) scan of the abdomen revealed a 10 cm X 8 cm X 8cms sized mixed density mass with few well-defined cystic lesions within. The wall of the cyst measured 2 to 3 millimeters. There was a well-defined calcified structure within one of the cyst, which resembled the vertebral body (Figure 1). This hyperdense structure was surrounded by fat density (Figure 2). The mass lesion was displacing the bowel loops and was situated anterior to the dorso lumbar spine, extending from the level of upper pole of the kidneys upto the level of anterior superior iliac spine. Rest of the abdominal viscera was unremarkable.
Discussion The term Foetus-in-fetu (FIF) was coined by Meckel1 in the 18th century and is defined as a parasitic twin found within the abdomen of its sibling. In 1809, Young reported the first case of foetus in fetu. Since then sporadic cases have been reported. Foetus in Fetu is discovered most commonly in infancy as a retroperitoneal mass.2 They may be totally asymptomatic.3 Symptoms, if present, are related to mass effect and include abdominal distension, feeding difficulties, emesis, jaundice and dyspnoea.3 In most cases FIF is present intra-abdominally in the upper part of the retroperitoneal space.4 Rare locations like cranial cavity, pelvis, scrotal sac, sacro-coccygeal region, mesentery and right iliac fossa are also reported.5 Usually they are one in number, but some cases of more than one have been reported.5 Many theories have been postulated to elucidate the exact pathogenesis of FIF. In earlier days, it was hypothesised that FIF results from a modified process of twinning and with a natural progression from normal to conjoined symmetrical twins through parasitic fetus and fetal inclusion and finally to teratoma.6 According to Willis,7 FIF arises from inclusion of monozygotic diamniotic twin within the bearer. Presence of vertebral axis (which develops from the primitive streak), appropriate arrangement of other organs or limbs with respect to the vertebral axis are the diagnostic features of FIF and these features help in differentiating this entity from the highly differentiated teratoma.7 Chromosome studies of the fetus show normal chromoso-mes identical to the host and the same blood group as their bearer.5 Serum alpha feto protein (AFP) levels may be elevated or may be normal. AFP levels may be elevated in 65-70% of patients and serum human chorionic gonadotropin is elevated in 50-65% of cases in patients with non-seminomatous tumours.3 FIF has characteristic imaging features. Plain abdominal radiographs may show a vertebral column and /or bony structures within a soft tissue mass.4 CT features are diagnostic of this entity. A mass comprising of round or tubular collection of fat around a central bony structure are typical CT findings in FIF.4 The identification of vertebrae or long bones within the lesion is essential for establishing the diagnosis. The exact extent of the mass and its relations with other abdominal structures are well elucidated on a contrast enhanced CT scan. This information aids in surgery, which is the treatment of choice for this condition. FIF shows varying degrees of organ system differentiation and deformity. Symmetric arrangement of the vertebral axis is required for diagnosis .The masses are often enclosed within membranes resembling amnion.3 Frequently vascular anasthamosis with the host vessels are identified.3 The closest differential diagnosis is a retroperitoneal teratoma. The distinction can be made from teratoma, as there is evidence of axial skeleton formation in FIF.3 It is a histologically proven benign entity but one case of malignant transformation and recurrence has been reported.3 The treatment of choice is complete surgical resection. In conclusion, the diagnosis of FIF should be considered in a child with a history of a slowly growing lump in abdomen in an appropriate clinical setting. A CT scan allows the prospective diagnosis of this very rare disease entity and aids in differentiation from the retroperitoneal teratoma.
References
This article is also available in full-text from http://www.jpgmonline.com/
© Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02044f1.jpg] [jp02044f2.jpg] |
| |||||||||

{kind=link}
{kind=link}