 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 2, 2002 pp. 142-148 Bone Graft Substitutes: Past, Present, Future Parikh SN Department of Orthopaedics, Children's Hospital Medical Centre, University
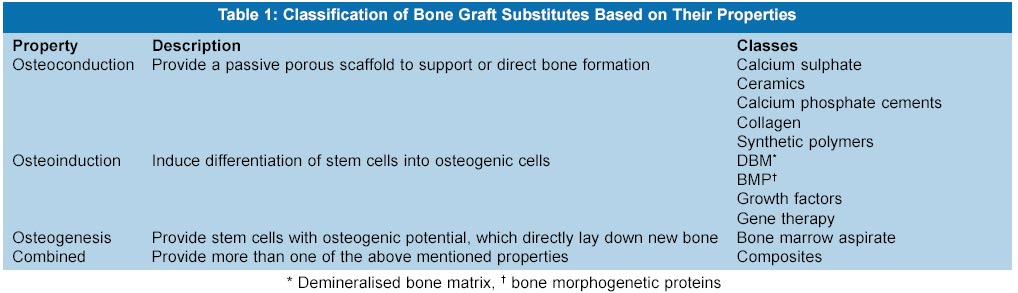
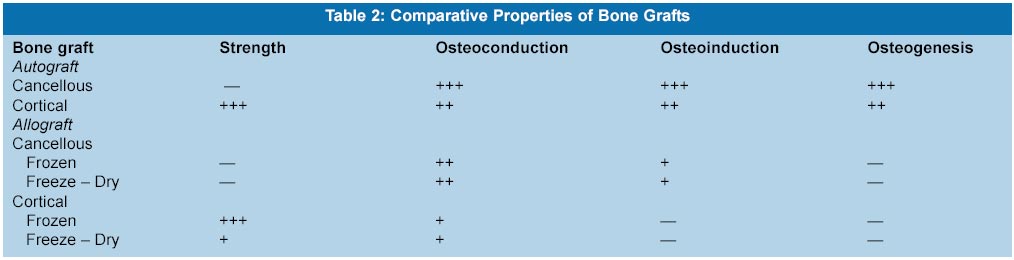
of Cincinnati, Cincinnati, OH 45229, USA. Code Number: jp02046 Abstract: Bone grafts are necessary to provide support, fill voids, and enhance biologic repair of skeletal defects. They are used by orthopaedic surgeons, neurosurgeons, craniofacial surgeons, and periodontists. Bone harvested from donor sites is the gold standard for this procedure. It is well documented that there are limitations and complications from the use of autograft, including the limited quantity and associated chronic donor site pain. Despite the increase in the number of procedures that require bone grafts, there has not been a single ideal bone graft substitute Scientists, surgeons, and medical companies, thus, have a tremendous responsibility to develop biologic alternatives that will enhance the functional capabilities of the bone graft substitute, and potentially reduce or eliminate the need for autograft. This article is an attempt to review the past and existing bone graft substitutes, and future directions of research. The historical data was extracted after thorough review of the literature. The data for the current concepts and future directions was compiled from the Internet, and from direct correspondence with medical companies. Since many products are undergoing clinical trials, and are yet not commercially available, their data cannot be found in literature. The main purpose of this article is to give the reader an idea about the existing market products and products likely to be available in near future. Key Words: Bone graft, bone graft substitutes, allografts, osteoconductive, osteoinductive, tissue engineering. Bone grafts are often necessary to provide support, fill voids, and enhance biologic repair of skeletal defects. Although autogenous bone is the gold standard that all alternatives must meet or exceed, autograft has significant limitations, including donor site morbidity, inadequate amount, and inappropriate form.1-3 These limitations have prompted increasing interest in alternative bone grafts. Allografts may be cancellous, cortical, or a combination of each. Though they are attractive sources, there are several problems encountered in using them, including the risk of disease transmission, immunogenicity,4 loss of biologic and mechanical properties secondary to its processing, increased cost, and non-availability world-wide due to financial and religious concerns. Consequently, significant efforts are being made to develop ideal bone graft substitutes. This article is an attempt to review the past and existing bone graft substitutes, and future directions of research. Bone grafts and their substitutes can be divided according to their properties of osteoconduction, osteoinduction, and osteogenesis (Table 1). A comparison of allograft and autograft bone, based on these properties, is shown (Table 2).
Osteoconductive Materials Osteoconduction is a three-dimensional process that is observed when porous structures are implanted into or adjacent to bone. Porosity alone, however, is not adequate for bone ingrowth. Porosity with interconn-ectivity is the most essential prerequisite. This is based on the three-dimensional interconnections between the lacunae in the bone that provide intercellular commu-nication. Although there are alternative views, the consensus of research indicates that the requisite pore size for bone ingrowth into porous implants is 100 to 500 mm, and the interconnections must be larger than 100 mm.6
Calcium Sulphate (Plaster of Paris) Gypsum, also referred to as Plaster of Paris, owes its name to a village just north of Paris. Although its external use for creation of hard setting bandages dates back to the seventeenth century, the first internal use to fill bony defects was reported in 1892 by Dressmann.7 The application of Plaster of Paris as a bone void filler, and the use of antibiotic-laden plaster in the treatment of infected bony defects, has been supported by various studies8-11 Calcium Sulphate (CaSO4) has long been used in its partially hydrated form. Medical grade calcium sulphate is crystallised in highly controlled environments producing regularly shaped crystals of similar size and shape. It possesses a slower, more predictable solubility and reabsorption. One such material is OsteoSet (Wright Medical Technology, Arlington, TN), which was approved by FDA in 1996. The material comes in the form of 30 and 48 mm pellets that typically dissolve in vivo within 30 to 60 days depending on the volume and location. The chief advantages are that it can be used in presence of infection and it is comparatively cheaper. Since it is bioabsorbable, it has inherent advantages over other antibiotic carriers, such as polymethylmethacrylate, which become a nidus for further infection after elution of the antibiotics, thus requiring a separate operation for removal from the surgical site. When this is combined with the eradication of dead space and the acidic environment created during its resorption, the compound can be an extremely effective treatment for acute bony infections with bone loss. However, three cases of inflammatory response and a single case of allergic reaction have been reported with the use of this compound.12
Calcium Phosphate (Ceramics) The earliest application of calcium phosphate salts was in the form of powders.13 The most commonly used calcium phosphate ceramics are hydroxyapatite (coral based or synthetic) and tricalcium phosphate, used in the form of implant coatings and defect fillers. These materials require high temperature and high pressure processing to produce dense, highly crystalline, bioinert ceramics, which are not mouldable intraoperatively and also have poor fatigue characteristics.
Porous Coralline Ceramics Chiroff et al14 first recognised that corals made by marine invertebrates have skeletons with a structure similar to both cortical and cancellous bone, with interconnecting porosity. There are two processes for manufacturing coralline implants One approach is to use coral directly in calcium carbonate form. These materials are called natural corals. The trade name for natural coral is Biocoral (Inoteb, Saint-Gonnery, France). The other process is Replamineform process that converts calcium carbonate to hydroxyapatite.6 Although there are hundreds of genera of stony corals, Porites and Goniopora are the only two genera meeting the required standards of pore diameter and interconnectivity.6 The exoskeleton of the genus Porites is similar to cortical bone and the exoskeleton of the genus Gonipora has a microstructure similar to cancellous bone. The products are trade named either Pro Osteon or Interpore porous hydroxyapatite (Interpore Cross International Inc, Irvine, CA), depending on the market to which they are directed. The number following the trade name designates the nominal pore diameter, either 500 or 200 mm A version of hybrid, coralline product (Pro Osteon 200R and 500R) has also been developed. It is a composite of calcium carbonate and calcium phosphate. A calcium phosphate layer, largely hydroxyapatite, is formed on the calcium carbonate pores. The thickness of the hydroxyapatite layer is adjusted to alter the resorption rates. In December 2001, a synthetic porous coated hydroxyapatite (PCH) bone substitute, OsSatura PCH (IsoTis NV, Bilthoven, The Netherlands) has been launched in Europe. It is a porous calcium phosphate scaffold with a biomimetic coating - first generation tissue engineered product. Its surface structure resembles that of natural bone, which makes it osteoconductive.
Tricalcium Phosphate (TCP) Like hydroxyapatite, TCP is bioabsorbable and biocompatible but its inadequate porosity, comparatively small grain size and its rapid dissolution (six weeks), makes it a poor bone graft substitute. Biocompatible and resorbable calcium phosphate cement - Norion Skeletal Repair System (Norion SRS, Norion Core, Cupertino, CA) has been introduced for augmentation of fracture repair. The chemical composition and crystallinity of the material are similar to those of the mineral phase of bone. It undergoes the same in vivo remodelling as normal bone to re-establish the bone morphology and strength. It appears to offer mechanical integrity for augmentation of fixation of sliding hip screw, pedicle screw, distal radius fracture, femoral and humeral neck fractures and recently, calcaneal fractures.15 Since it is applied in a liquid stage as a paste, it may be difficult to control; it may leak into the joint or prevent sliding of a sliding device.16,17 a-BSM - Bone Substitute Material (ETEX Corp, Cambridge, MA) is a poorly crystalline calcium phosphate cement with favourable absorption characteristics and easy intra-operative handling characteristics.18 It is hydrated with saline to form a workable paste, which remains formable for hours at room temperature but hardens within 20 minutes at physiologic body temperature. It is marketed in Europe as Biobon (Biomet Merck, The Netherlands).
Collagen Type I collagen is the most abundant protein in the extra-cellular matrix of bone. It has a structure that is conducive to promoting mineral deposition and it binds the noncollagenous matrix proteins, which initiate and control mineralisation by itself. Collagen functions poorly as a graft material, but when coupled with bone morphogenetic proteins, osteoprogenitor precursors, or hydroxyapatite, it enhances incorporation of grafts significantly. Collagraft (Zimmer, Warsaw, IN) is a composite of suspended fibrillar collagen and a porous calcium phosphate ceramic, in a ratio of 1:1. The fibrillar collagen is highly purified collagen obtained from bovine dermis. Autologous bone marrow aspirate can be added to these materials or it can be mixed with autologous bone as a bone graft extender. It does not offer structural support by itself and its movement may be difficult to control.19,20 Healos (Orquest, Mountain View, CA) is a mineralised collagen sponge, launched in Europe for clinical use in 2000. Each microscopic Type I collagen fibre is coated with hydroxyapatite These fibres are then fabricated and cross-linked into a three-dimensional, continuously porous and stable final format. It can be mixed with bone marrow aspirate to provide osteogenic and osteoinductive potential. Another novel bone-inducing protein, MP52, is integrated with Healos bone graft substitute, to induce bone formation. MP52 is a member of the BMP family. This product, Healos/MP52, is expected to improve the overall success rate of current spinal fusion procedures.
Nonbiologic Substrates Considerable interest has developed in creating osteoconductive matrices using nonbiologic materials. Degradable poly-mers, bioactive glasses, and various metals have been studied. The advantage of nonbiologic materials includes the ability to control all aspects of the matrix, avoidance of immunologic reaction, and excellent biocompatibility. Polylactic and Polyglycolic acid polymers have been used extensively as suture materials, and biodegradable fracture fixation implants. These materials have the advantage of being assembled in various forms and can be integrated with growth factors, drugs, and other compounds to create multiphase delivery systems. Immix (Osteobiologics Inc, San Antonio, TX) is a synthetic bone graft scaffold, tissue-engineered from amorphous D, L-Polylactide-co-glycolide (PLG), and is designed to resorb within 12- 20 weeks following implantation. They provide a porous architecture for the ingrowth of new bone and then fully degrade. A variety of porous metal surfaces and coatings have been used as surfaces for bone ingrowth intended to fix prosthetic joint replacement components to bone. These include sintered cobalt-chrome beads, titanium alloy fibre metals, and plasma-sprayed surfaces. New metallurgy techniques are creating metallic matrices of much greater porosity. Tantalum can be fabricated as metallic foam-like structure with interconnecting pores, which allows exceptionally rapid and complete ingrowth. Hydroxyapatite coating of metal surfaces enhances ingrowth and direct bonding of bone to porous surface.21,22 Essentially, these coatings can be used on implants with relatively simple surface geometry and use excessive high temperatures. This means that it is difficult to coat implants with complex surface geometry (e.g. porous surface) and that no biologically active agents can be added to the coating during the spraying process. A technology has been developed by IsoTis NV (Bilthoven, The Netherlands), that allows the growth of a thin layer of bone-like ceramic over medical devices.23 The calcium phosphate coating is grown from an aqueous fluid at ambient temperatures. In contrast to conventional technologies, these `biomimetic' coatings can be applied on to surfaces with complex geometry, and active agents such as growth factors or antibiotics can be co-precipitated. This creates the possibility of using these coatings as slow release systems.24
Osteoinductive Agents Osteoinductive agents are bone graft substitutes, generally proteins, which induce differentiation of undifferentiated stem cells to osteogenic cells or induce stem cells to proliferate. Several osteoinductive agents have been identified. Among these compounds are transforming growth factor (TGF-b),25 bone morphogenetic proteins (BMPs),25-28 fibroblast growth factors (FGFs),29,30 insulin-like growth factors (IGFs),31 and platelet-derived growth factors (PDGFs).32
Demineralised Bone Matrix (DBM) Since the initial studies performed by Urist,33 the osteoindu-ctive capacity of DBM has been well established.34 DBM is produced by the acid extraction of human cortical bone and the components of the bone that remain behind include the non-collagenous proteins; bone osteoinductive growth factors, the most significant of which is BMP; and type I collagen. DBM provides no structural strength, and its primary use is in a structurally stable environment. Hydroxyapatite, autograft, allograft or bone marrow cells may be added to DBM. A carrier may be added to DBM to improve its handling characteristics and mechanical properties (Table 3). DBM obtained from allogeneic human cortical bone shows variable efficacy and osteoinductive index. A reproducible and rapid bioassay (AlloSource bioassay, AlloSource, Centennial, Colorado), using human cells of osteoblastic lineage, SAOS-2 cells, has been developed to correlate the activity of DBM.35
Bone Morphogenetic Proteins The BMPs (BMP 1-7) are low-molecular-weight non-collagenous glycoproteins that belong to an expanding TGF-b superfamily of atleast 15 growth and differentiation factors. They make up only 0.1% by weight of all bone proteins. Unlike DBM, which is a mixture of BMPs and immunogenic, non-inductive proteins, the pure form of BMPs is non-immunogenic and non-species specific. Currently single BMPs are available through recombinant gene technology, and mixtures of BMPs are available as purified bone extracts for clinical studies. The recombinant human BMPs extensively studied are rh-OP-1 (osteogenic protein 1), rh-BMP-2 (Genetics Institute, Cambridge, MA) and rh-BMP-7 (Creative Biomolecules, Hopkinton, MA). In October 2001, approval was granted by the FDA for recombinant OP-1 implant, for use as an alternative to autograft in recalcitrant long bone nonunions. This is the first BMP approved for clinical use in the US. The approved product, OP-1 Implant (Stryker Corporation, Kalamazoo, MI) is a combination of rh-OP-1 and a bovine collagen carrier. The rh-OP-1 is derived form a recombinant Chinese Hamster Ovary cell line, and the bovine collagen is derived from the diaphyseal bone and is primarily Type I. It is a white lyophilised powder, which has to be reconstituted with two to three ml of saline, prior to use. It forms a paste which is then surgically implanted at the fracture site. The osteogenic activity of OP-1 has been proven in a validated critically-sized fibular defect in human subjects.36 In November 2001, the first two-year results of a clinical study of rh-BMP-2 (Genetics Institute, Cambridge, MA), were presented at the North American Spine Society meeting. InFuse (Medtronic Somafor Danek, Minneapolis, MN) is a new investigational material containing genetically engineered recombinant human BMP-2 with a collagen sponge carrier. The results of the clinical study for the evaluation of InFuse bone graft substitute along with titanium cages for lumbar spinal fusion were promising. Earlier, a prospective randomised controlled human clinical pilot trial had shown definite evidence of osteoinduction with the use of rh-BMP-2 in inter-body fusion cages for single-level lumbar degenerative disc disease.37
Other Growth Factors Besides the growth factors expressed from the extra-cellular matrix of the bone (DBM, BMP), there are other factors in the circulating blood, which play a role in bone healing. TGF-b is the most extensively studied growth factor in the field of bone biology. It comprises an entire family of molecules that includes the BMPs. In 1994, Genentech, Inc (San Francisco, CA) was issued the patent for developing TGF-b through recombinant technology. This covered the nucleic acids, vectors and host cells used for production of recomb-inant TGF-b. In an animal study, it was found that BMP, and not TGF-b, enhanced bone formation38. PDGF is another factor whose effect was studied on the bone healing of unilateral tibial osteotomies in rabbits. It was concluded that PDGF had a stimulatory effect on fracture healing.32 Autologous Growth Factors AGF (Interpore Cross International Inc, Irvine, CA) is an innovative concept. AGF gel is obtained from the buffy coat of the blood collected in the cell saver during surgery, through the process of centrifugation. It is rich in growth factors, especially TGF-b and PDGF. Approximately 20 ml of AGF is derived from 500 ml of blood in ten minutes and it is placed at the fracture site. Bovine-derived bone morpho-genetic protein extract (NeOsteo, Intermedics Orthopaedics, Denver, CO) is a cocktail of growth factors and is currently being evaluated for its role in human spine fusion and periodontal repair. It can be combined with either DBM or a coralline calcium carbonate carrier. Basic fibroblast growth factor (bFGF) is produced locally in bone during the initial phase of fracture healing and is known to stimulate cartilage and bone-forming cells.29 Ossigel (Orquest, Mountain View, CA) is a formulation of bFGF and hyaluronic acid (Hy). It is delivered as a single minimally invasive injection into the fracture site. Hy is a viscoelastic polymer found throughout the body that cushions and protects soft tissues. The synergistic combination of bFGF and Hy appears to accelerate the fracture healing process and underscores the importance of using an appropriate carrier not only for bFGF but also possibly for other growth factors. Ossigel is currently under clinical trials in the US and Europe.
Bone Marrow Aspirate Bone marrow has been used to stimulate bone formation in skeletal defects and nonunions.39 The major advantage of this technique is that it can be performed percutaneously, without almost any patient morbidity. The bone marrow is aspirated with a large bore needle from the iliac crest and injected percutaneously with fluoroscopic guidance into the nonunion site. Approximately one of every 100,000 nucleated cells aspirated from bone marrow is a stem cell. Centrifugation of aspirated bone marrow at 400 times gravity for ten minutes separates the marrow cells from plasma and preserves the osteogenic potential of the cells, decreasing the volume of material injected.40 It may be possible to increase the proliferation and speed-up differentiation of stem cells by exposing them to growth factors,41 or by combining them with collagen.19
Future Directions Tissue engineering Advances in tissue engineering and the integration of the biological, physical, and engineering sciences, will create new carrier constructs that regenerate and restore functional state. These constructs are likely to encompass additional families of growth factors, evolving biological scaffolds, and incorporation of mesenchy-mal stem cells. Ultimately, the development of ex vivo bioreactors capable of bone manufacture with the appropriate biomechanical cues will provide tissue-engineered constructs for direct use in the skeletal system. VivescOs (IsoTis, Bilthoven, The Netherlands) is a tissue-engineered bone, developed for application in revision surgery, spinal fusion and dental implants. The bone marrow cells are harvested from the patient, then multiplied in culture, shaped in appropriate structure on a scaffold, and implanted into the patient. The process takes 4 weeks. This fully tissue-engineered bone is expected to be launched in 2004.
Gene Therapy Once considered a fantasy, there is a compelling evidence to support the utility of gene therapy for bone induction in humans.42 Studies have successfully demonstrated several safe, effective strategies to form new bone via gene therapy in animals. Gene therapy involves the transfer of genetic information to cells. When a gene is transferred to a target cell, the cell synthesises the protein encoded by the gene. The duration of protein production that is required and the anatomic location where the protein must be delivered determine the strategy employed. The gene therapy used for bone induction is short-term, regional therapy. The gene can be introduced directly to a specific anatomic site (in-vivo technique) or specific cells can be harvested from the patient, expanded, and genetically manipulated in tissue culture, and then reimplanted (ex-vivo technique). The vehicle for gene delivery can be either viral (adenovirus, retrovirus) or non-viral (liposomes, DNA-ligand complexes). The gene can be selectively transferred to a targeted cell (osteoblast, fibroblasts) at the bone induction site.
References
This article is also available in full-text from http://www.jpgmonline.com/
© Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02046t3.jpg] [jp02046t2.jpg] [jp02046t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}