 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
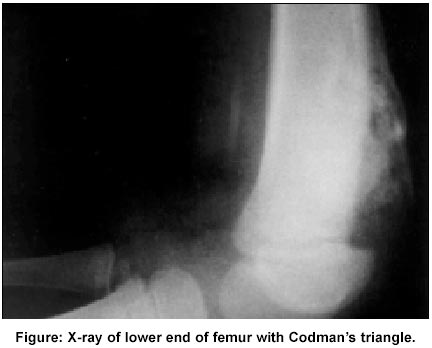
Journal of Postgraduate Medicine, Vol. 48, Issue 2, 2002 pp. 157-158 Letter to the Editor Codman's Triangle in Tubercular Osteomyelitis Desai RV, Jain V, Katariya S Departments of Radiodiagnosis and Pediatrics, Postgraduate Institute of medical education and Research, Chandigarh -160 012, India. E-mail: vivsem@yahoo.com Code Number: jp02052 Sir, An eight-year-old male child presented with prolonged history of low-grade fever and a progressively increasing swelling on left lower thigh. His grandmother was treated for pulmonary tuberculosis a year back. He had cervical lymphadenopathy, hepatosplenomegaly and bronchial breath sounds and crepitations in right infra-axillary area. The thigh swelling was firm, mobile and tender without erythema or warmth. The movements of the left knee joint were normal. Investigations showed haemoglobin concentration of 7.6gm%, total leucocyte count of 6200/mm3 with polymorphs 73%, lymphocytes 26%, and eosinophils 1%. Erythrocyte sedimentation rate was 125 mm at the end of one hour. Tuberculin test produced 15x20 mm induration. Chest X-ray showed right middle and lower zone consolidation with mediastinal enlargement. ELISA for retrovirus was negative. X-ray of lower end of left femur (Figure) showed anterolateral cortical erosion with subperiosteal new bone formation in the form of Codman's triangle. Medullary bone sclerosis was also seen. Excisional biopsy of swelling revealed epitheloid cell granuloma, caseous necrosis and new bone formation. Stain for acid-fast bacilli were positive and culture grew tubercle bacilli. He was started on anti-tubercular treatment, to which he has clinically responded. Mycobacterial infections of the limbs may closely resemble malignancy.1 Radiological findings associated with tuberculosis of bones and joints include osteopenia, narrowing of the joint space, soft-tissue edema with little periosteal reaction, cysts in bone adjacent to joint space, and subchondral erosions.2 Codman's triangle, classically described in osteosarcoma, is an isolated cuff (triangle) of reactive subperiosteal new bone at the boundary of any benign or malignant mass that rapidly elevates the periosteum.3 Thus, though demonstration of Codman's triangle requires pathological confirmation to rule out a tumor, it may also develop following rapid displacement of periosteum by blood or any infectious exudates, as occurs with acute osteomyelitis or post-traumatic intraperiosteal hemorrhage.3 Unlike acute pyogenic infection, the natural history of tuberculous lesion is that of a subacute or chronic infection. Thus, in tuberculosis of long bones there is no evidence of reactive sclerosis or periosteal new bone formation. This is in contrast to acute osteomyelitis, where clinical symptoms precede radiological changes by two weeks and the first radiological sign is usually that of the periosteal new bone formation.4 Thus this case showed unusual radiological features of increased bone density and Codman's triangle. Though the child did not have immunodeficiency, he did have severe systemic features of the disease (hepatosplenomegaly, anemia and presumed rapidly progressive pneumonia) suggesting that he was relatively immunocompromised and perhaps therefore this primarily progressive tubercular infection appeared so radiographically aggressive in the bone (resulting in the formation of Codman's triangle). In the present case Codman's triangle showed relatively solid non-laminar new bone indicating that although the lesion may have been aggressive initially, it was less so at the time of imaging.
Desai RV, Jain V, Katariya S Departments of Radiodiagnosis and Pediatrics, References
This article is also available in full-text from http://www.jpgmonline.com/
© Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02052f1.jpg] |
| |||||||||

{kind=link}