 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 3, 2002 pp. 179-181 Azithromycin as Treatment for Cryptosporidiosis in Human Immunodeficiency Virus Disease Kadappu KK, Nagaraja MV, Rao PV, Shastry BA Department of Medicine, Kasturba Medical College Hospital, Manipal, Karnataka
576119, India. Code Number: jp02062 Abstract: Background: Cryptosporidiosis caused by the protozoa Cryptosporidium, is the common cause of diarrhoea in Acquired Immune Deficiency Syndrome (AIDS). Aim: To study the efficacy of short-term azithromycin in the management of cryptosporidiosis. Settings and Design: Randomised, controlled trial. Material and Methods: All consecutive patients infected with Human Immunodeficiency Virus (HIV), who were positive for cryptosporidial oocysts were taken for this prospective randomised study. Result: Short-term azithromycin treatment for cryptosporidial diarrhoea in AIDS patients was associated with good clinical improvement but parasitological benefit was doubtful. All 13 patients, who had symptoms of cryptosporidiosis, symptomatically improved with 5 days of treatment with azithromycin and became asymptomatic after 7 days of antibiotic, but stool sample was positive for cryptosporidium even after 7 days of therapy. After 14 days of treatment with azithromycin in 13 patients, in five patients stool was free of cryptosporidial oocyst. The drug was well tolerated in all the patients. Conclusion: Short-term azithromycin can be used as a safe and effective treatment for symptomatic Cryptosporidiosis but not effective in eradicating Cryptosporidial infection. (J Postgrad Med 2002;48:179-181) Key Words: Cryptosporidiosis, Azithromycin, AIDS. Cryptosporidiosis is an intestinal and pulmonary disease caused by the protozoan Cryptosporidium. Its most common manifestation in mammalian species is enteric disease, which in immunocompetent hosts is self-limiting but can be life-threatening in hosts with suppressed immune function.1,2 Cryptosporidiosis is the reported cause of diarrhoea in 15 to 40% of adults with AIDS, the proportion of affected patients varying by geographic location.3,4 As the number of AIDS patients increases, there will be an increasing need for effective therapy against this disease. In general, no specific therapy for cryptosporidial infection has been identified.4-9 Rifabutin, paromomycin and azithromycin10-12 were tried against cryptosporidium in immunocompromised individuals. As azithromycin showed promising activity in animal models and other immunocom-promised humans to treat cryptosporidial infection and rifabutin is not easily available in India, azithromycin was used in this study. Even though cryptosporidiosis is the commonest intestinal parasitic infection in HIV disease13 in India, no study has been done in India about its treatment.
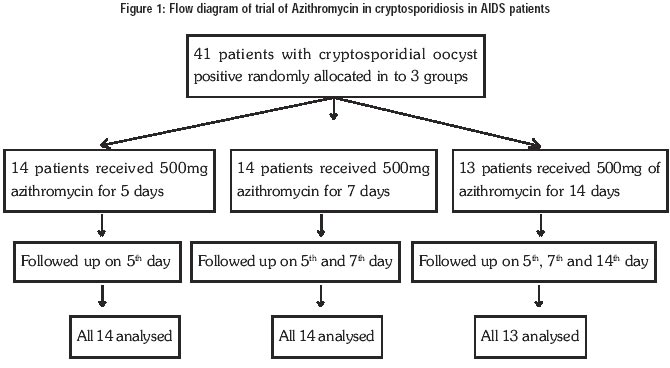
Material and Methods A total of 65 (60 males and 5 females) consecutive patients who were diagnosed as AIDS patients from August 1997 to August 2001 were screened for cryptosporidial oocyst in their stool. All patients, who were positive for cryptosporidial oocyst in their stool, were candidates for inclusion in the study. Patients with chronic diarrhoea for more than 2 months or profuse watery diarrhoea for 4 days or diarrhoea with intermittent fever for 2 weeks duration were considered as symptomatic. Patients who were already on any anticryptosporidial or antidiarrhoeal medications were not considered in this study. The patients were aged between 22 and 63 years. Written informed consent was taken before the treatment. CD 4+ count was done in 17 patients, who are willing for highly active anti-retroviral therapy as practised in our hospital. Out of these 17 patients, 11 patients were positive for cryptosporidial oocyst. CD4+ count ranged from 51 to 220. Thirty-eight patients had tuberculosis, 22 had oesophageal candidiasis, 13 patients had pneumocystitis pneumonia, 8 had cryptococcal infection and 3 patients had giardiasis and cytomegalo virus infection. All patients were on concurrent treatment for coexisting disease. Stool was collected and concentrated sediment was preserved in 10% formalin. Stools were processed by modified acid-fast staining14 to detect cryptosporidia. Stool samples were examined by the same microbiologist on the first day, 5th day, 7th day and 14th day of the study, who was kept blind from this study groups. Stool samples were also examined for bacteria, microsporidia, and other parasites like Giardia lamblia. A detailed history was taken and a thorough clinical examination was performed. These 41 patients were randomly divided into 3 groups. Group 1 and group 2 had 14 patients each and both groups had 4 symptomatic patients. Remaining 13 were in group 3 in which 5 patients were symptomatic. Patients in group I were given azithromycin 500mg once daily for 5 days. Group II received the same dose of azithromycin for 7 days and group III received it for 14 days. No concomitant antidiarrhoeal drug was administered. Clinical assessment was done and haematological and liver function tests were monitored on the 5th and 14th days of the therapy. Symptomatic improvement was defined as more than 50% reduction in baseline stool frequency with a feeling of well-being. Asymptomatic improvement was defined as cessation of diarrhoea with normal body temperature.
Results Of 41 patients, majority were asymptomatic (Table 1). Five patients had persistent diarrhoea. Four had watery diarrhoea and yet another 4 had prolonged fever with intermittent diarrhoea. All patients who had symptoms of cryptosporidiosis improved after 5 days of treatment with Azithromycin and became asymptomatic after 7 days of antibiotic therapy. All patients were positive for cryptosporidial oocysts in stool even after seven days of Azithromycin therapy. The stool of five patients who received antibiotics up to 14 days became negative for cryptosporidial oocyst. No patient had any untoward drug reaction during the study.
Discussion In immunocompetent patients, cryptosporidiosis is a self-limiting infection. However, in an immunocompromised individual, therapy may be critical, even though there is no reliable curative treatment for cryptosporidiosis. From initial studies, it appears that paromomycin, a poorly absorbed aminoglycoside antibiotic, is a well-tolerated and an easily administered agent for management of cryptosporidiosis. However, despite encouraging anecdotal data, the drug does not appear to be uniformly effective in oocyst eradication and / or resolution of symptoms and, as with the majority of AIDS therapies, seems to require prolonged and indefinite course of therapy.11 Spiramycin, a macrolide antibiotic showed initial promise in Europe, but efficiency was not demonstrated in controlled clinical trails in HIV infected patients.15 Azithromycin, another macrolide, was used in cryptospo-ridiosis both in immunocompromised animals and humans with variable efficacy.10-12 Azithromycin was found to be highly effective in the prevention and treatment of experimental cryptosporidial infection in the ileum of immunocompromised rats and its activity was dose- dependent.10 In a study on 13 patients, it was showed that long-term, low dose azithromycin was well-tolerated and may induce stable remission of chronic cryptosporidiosis in patients with AIDS.3 In our study, out of 65 AIDS patients, 41 were positive for cryptosporidial oocyst, which is much higher than the worldwide incidence. This may be attributed to the poor personal hygiene, as most of our patients were from very low socio-economical strata. We had 5 patients with CD4+ count more than 180 who were asymptomatic passers of cryptosporidial oocysts. 2 of them were in group II and received 7 days of azithromycin and stool was still positive for oocyst. Another 3 patients received 14 days of azithromycin and their stool became negative for oocyst. Two patients with less than 180 CD4+ count (one with a count of 165 and another with 168) had stool negative for cryptosporidial oocyst after 14 days of azithromycin therapy. Therefore, the response should be presumed to be due to azithromycin therapy rather than the immunological status of the patient. Relapses of cryptosporidiosis in these patients were not assessed, as the aim of the study was to assess the short-term efficacy of azithromycin therapy in the management of cryptosporidiosis. As HIV is emerging as a major health problem in India and studies in India show 94.4% of intestinal opportunistic infection in HIV due to cryptosporidium species13, we should have a cheaper and safe medication against this protozoan. Even though rifabutin is a good drug against cryptosporidium, it is costly and sparsely available in India. Moreover, as most of our HIV patients harbour tuberculosis, use of rifabutin without ruling out tuberculosis, may result in a valuable drug against tuberculosis being lost due to drug resistance. In conclusion, azithromycin can be used as a safe and effective antiprotozoan drug against cryptosporidiosis in HIV patients. Further study is required assess the efficacy, dosage and duration of azithromycin as prophylaxis against cryptosporidiosis in HIV patients.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02062t1.jpg] [jp02062t2.jpg] [jp02062f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}