 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 3, 2002 pp. 191-196 A 34-year-old Renal Transplant Recipient with High-Grade Fever and Progressive Shortness of Breath Soman R, Vaideeswar P,* Shah H,** Almeida AF** Department of Medicine, PD Hinduja National Hospital and Medical Research Centre,
Mahim, and Departments of Pathology, * Code Number: jp02065
A 34-year-old man was referred for evaluation of renal failure. The illness had started with a 2-month history of easy fatiguability, nausea and vomiting which was followed by puffiness of face and oedema feet and a decrease in urinary output. He did not provide a long-standing history of renal symptomatology or that of any systemic disorder. His past medical history revealed a fully treated tuberculous lymphadenitis, 8 years prior to presentation and a history of multiple unprotected sexual encounters with penile ulcerations on 3 occasions, treated with unspecified medications. He was a chronic smoker, but a teetotaler. On presentation, he had clinical features of uncontrolled hypertension (170/116 mm of Hg) with grade III hypertensive retinopathy, facial and pedal oedema and cardiac failure. Investigations revealed a haemoglobin concentration of 7.6 gm%, mild leucocytosis (neutrophils 80%, lymphocytes 20%); urine protein 2+ with 12-15 red blood cells per high power field; Blood urea nitrogen 65 mg% and creatinine 14.4 mg%. Sonographic examination revealed normal sized kidneys. A provisional diagnosis of rapidly progressive renal failure was made and a renal biopsy was performed. It revealed 8 glomeruli, 6 showing global sclerosis and one with partial sclerosis. Interstitial fibrosis and tubular atrophy existed. A diagnosis of chronic renal failure secondary to a chronic glomerulonephritis was made. This non-diabetic, hypertensive patient, was initiated on maintenance hemodialysis in preparation for a live related donor transplant. He received antihypertensive agents (nifedipine retard and alpha methyl dopa), oral iron supplements, and recombinant human erythropoietin subcutaneously. He did not receive blood transfusions and was negative for viral markers (HbsAg, CMV IgM and CMV IgG). Hepatitis B vaccination resulted in seroprotective titres of anti-HBs antibodies. Live related donor renal transplant was performed about ten months later. His elder sister, a haplotype-matched organ donor, was found to be medically and emotionally suitable for organ donation. She, too, was negative for viral markers. Brisk diuresis was noted from the transplanted kidney. Renal functional improvement was noted for the first two weeks on an immunosuppressive regimen of azathioprine and prednisolone. Towards the end of the third week, he had an acute rejection episode (creatinine rose from a baseline of 1.5 mg% to 2.2 mg%), diagnosed on fine needle aspiration of the graft and successfully treated with pulse methyl-prednisolone boluses. The patient also developed an episode of urinary tract infection, which was treated successfully. The patient made satisfactory progress (Serum creatinine level returned to baseline value of 1.5 mg%, weight gain of 3 kg) and he returned to his job 4 months after transplant surgery. Six months after transplant surgery; the patient complained of abdominal distension and discomfort, flatulence and a dry cough. Examination revealed a normotensive patient with oral thrush but no other systemic abnormalities. Renal parameters were stable; urinalysis showed mild proteinuria with occasional white cells and the liver function tests were normal. For the first time, post-prandial glucose levels were found to be elevated. Fluconazole was given for oral thrush, his diabetes was controlled with the help of dietary restriction and tolbutamide and anti-hypertensive drugs were continued. He was sent home on azathioprine (2.5 mg/kg) and prednisolone (10 mg). He returned to the hospital a couple of weeks later with a two to three day history of high-grade fever, progressive increasing shortness of breath not associated with chest pain, cough or haemoptysis. There were no abdominal complaints. Examination revealed tachypnoea, tachycardia and blood pressure of 120/80 mm Hg. Crackles were heard widely over the chest, being more extensive over the infra-scapular area. Investigations showed a haemoglobin concentration of 14 gm%; total leucocyte count 7660/cmm with 70% neutrophils, 25% lymphocytes, and 5% eosinophils. The platelet count was 90,000/cmm. BUN (34 mg%) and serum creatinine levels (1.9 mg%) were elevated over previous values. Serum electrolyte levels were normal. Arterial blood gas analysis revealed: pO2 46 mm Hg, pCO2 31 mm Hg and SaO2 65%. Chest skiagram showed bilateral confluent reticulonodular shadows without mediastinal lymphadenopathy. Sputum examination showed 2-3 epithelial cells, 6-8 macrophages and 6-7 pus cells per high power field. Peripheral blood smear was negative for malarial parasites and so also were blood and urine cultures (bacterial and fungal). HBsAg was negative, no HIV antibodies were detected by ELISA and CMV IgM and CMV IgG titres, though positive, did not show a four fold increase. The patient was started on cefotaxime, amikacin and co-trimoxazole with simultaneous reduction of the dosage of prednisolone and azathioprine. High flow oxygen therapy showed temporary improvement of pO2. The arterial desaturation worsened over the next 18 hours requiring ventilatory assistance. Arterial blood gases improved marginally on a FiO2 of 0.6. Swan Ganz catheterisation revealed right atrial pressure 7/5, left 10/12, pulmonary pressure 12/23, Pulmonary capillary wedge pressure (PCWP) 12. On the next day, the condition worsened with persistent fever, onset of hypotension with warm extremities, deteriorating sensorium, leucopenia and thrombocytopenia. Arterial desaturation persisted. Empirical acyclovir therapy, in the absence of ganciclovir, was instituted to cover for probable CMV infection. A diagnostic procedure was performed. The patient continued to deteriorate and succumbed to this illness on the following day.
Clinical Discussion (By R. Soman) In summary, this is a 34 year old male, 6 months post-renal transplant, on steroids and azathioprine who developed an acute onset fever, dyspnoea, tachypnoea, bilateral basal crepitations, bilateral confluent reticulonodular shadows, marked arterial hypoxaemia, wide A-a gradient of 334, normal PCWP, PA, RA pressures. Although the respiratory symptoms are acute, in reality, the illness appears to have begun 15 days before with GI disturbances. The other distinguishing feature in this case is eosinophilia.
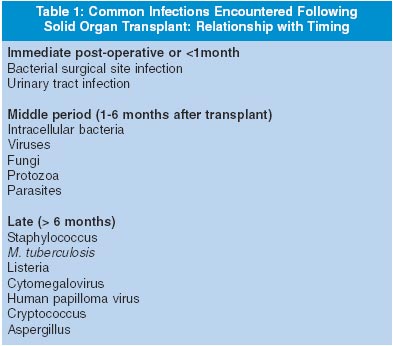
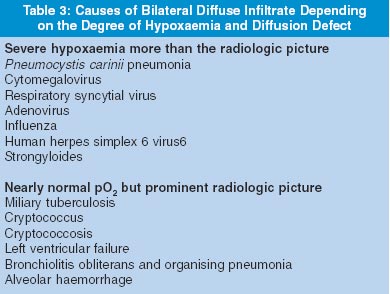
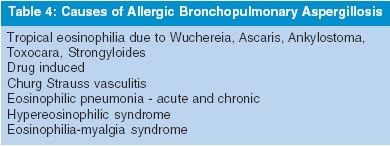
Are any clues available from the pre Solid Organ Transplant (SOT) history? The patient had tuberculous adenitis and probably had syphilis. He had presented with a Rapidly Progressive Glomerulonephritis (RPGN), the pathologic correlate of which is crescentic GN. The patient did not have any evidence of infectious processes or vasculitis that could give rise to crescentic GN or have a bearing on the present illness. The present pneumonic process appears to be an infectious disease because he has an immunocompromised status; the illness was of acute/subacute onset with fever and had a rapid downhill course. However, the clinician may be overwhelmed by exotic infectious disease possibilities and may overlook easily treatable non-infectious entities that mimic pneumonia. Those under consideration would be pulmonary thrombo-embolism (PTE), congestive or left ventricular failure (CHF/LVF) but has normal haemodynamic parameters; ARDS is present but one is still in search of the inciting cause. Bronchiolitis obliterans and organising pneumonia (BOOP) is a pathological diagnosis, a non-specific reaction of the lung to insults by infection, vasculitis, or inhaled antigens. In this condition, there is bilateral alveolar infiltration which may be migrating or transitory and which responds to steroids. Vasculitis, drug, oxygen, radiation-induced pneumonitis, alveolar haemorrhage, leucoagglutinin reaction and lymphangitic spread of malignancy are the other non-infectious mimics of pneumonia. There is nothing in the case record to support any of these possibilities. The type of infections in an immunocompromised host depends on the type of immunosuppression, degree of immunosuppression, the specific agent used (For example, OKT3 is associated with CMV infection), the time of infection in relation to the onset of immunocompromised state, presence of prior latent infection, prior immunity to specific organisms (for example, immunity against toxoplasmosis, CMV, varicella), the prophylaxis for opportunistic infections received, co-infection with CMV and Pneumocystis carinii or human herpes virus-6 (HHV-6). Since this patient presented at 5½ months post-transplant, he is likely to have infections of the middle or late period. Infections in immunocompromised hosts are difficult to evaluate. The usual symptoms, signs, radiologic, serologic and hematologic alterations may not develop. The law of parsimony does not hold good. Co-infections, multiple and sequential infections can occur. Non-infectious mimics occur. Current diagnostic tests are not rapid, sensitive or specific enough to identify or exclude a microbial cause. Prompt treatment is needed. A diagnostic algorithm for pulmonary infections can be based on the clinical signs and symptoms, the acuteness of the process, the radiologic picture and the degree of hypoxaemia (Table 2 and 3). Thus far, I have concentrated on the patient being immunocompromised. In which direction would one be led, if the patient, in addition, has pulmonary infiltrates with eosinophilia (PIE)? Allergic Bronchopulmonary Aspergillosis (ABPA) is the condition to be considered here. ABPA mainly presents as asthma, which is difficult to treat. Most of the conditions causing ABPA (Table 3) are steroid responsive, or are unlikely to worsen while on steroids, with the exception of Strongyloides infection, which can multiply in the human body, especially under the influence of steroids. Now, let us discuss differential diagnosis of closely matching entities: Tuberculosis as a reactivation disease is quite common following Solid Organ Transplant. The most common presentation is that of a focal infiltrate on the chest radiograph though a miliary picture could also occur. This patient had tuberculous lymphadenitis in the past. Tuberculosis, however, does not produce such severe hypoxaemia or such a rapid downhill course as was manifest in this case. Nocardiosis presents with reticulonodular shadows or lobar consolidation. The abscess may spread to adjacent tissues or manifest as a cerebral abscess. Nocardia are Gram positive, beaded, branching rods, partially acid fast. This patient, however, was on co-trimoxazole and that is the treatment of choice for Nocardiosis. Cryptococcosis presents with bilateral diffuse infiltrate but the pulmonary involvement is usually asymptomatic. Meningitis, skin and subcutaneous nodules are the common modes of presentation. Aspergillosis, presents with multifocal or cavitating infiltrate and is more common with neutropenic patients. Candida rarely causes a primary lung infection. Geographically limited endemic fungi such as histoplasm-osis, coccidiodomycosis and blastomycosis produce reticulo-nodular infiltrate, mediastinal fibrosis, erythema nodosum, skin nodules and hilar adenopathy. The last was specifically noted to be absent in this case. These infections are diagnosed on biopsy of involved tissues. Legionella usually has multifocal consolidation, diarrhoea, hyponatremia, central nervous system abnormalities, hypophosphataemia and abnormal liver function tests. Mycoplasmal infections are characterised by haemolysis, erythema multiforme and involvement of the central nervous system and ear involvement. Chlamydial infection is characterised by sore throat, hoarseness and a wheeze. Pneumocystis carinii pneumonia (PCP) manifests with fever, dyspnoea, cough, bilateral basal crepitations and a chest skiagram with no abnormal findings or subtle infiltration or confluent reticulonodular or cystic shadows. Significant hypoxaemia and high LDH levels are associated with this infection and the demonstration of the organism on sputum, bronchoalveolar lavage (BAL) or in a transbronchial biopsy is diagnostic. All the features in the patient can be explained on the basis of PCP. But the patient continued to worsen despite cotrimoxazole, which is the drug of choice for PCP. Cytomegalovirus infection: Fifty percent of SOT recipients develop symptomatic disease. Recipients who are CMV negative and those who have received anti-lymphocyte globulin (ALG) or OKT3 are at risk. IgG CMV became positive in this case which indicates infection through the donor organ, blood product, or contact with a CMV shedder. The usual features of CMV infection are cholangitis, hepatitis, colitis, cytopenias, retinitis and immunosuppressive effect leading to co-infection with Pneumocystis carinii, Human Herpes Virus 6 (HHV 6) and bacteria. The diagnosis of CMV disease is based on finding CMV inclusions in affected tissue, PP65 CMV antigen in white cells and PCR CMV DNA. There is nothing against CMV infection in this case. Adenovirus produces interstitial pneumonitis, colitis, hepatitis and cystitis. It is treated with ribavarin, vidarabin, ganciclovir but the success rate is low. HHV 6 produces fever, leucopenia, interstitial pneumonitis and encephalitis. CMV can be a co-pathogen. HHV6 is an inducer of cytokines, rejection and fungal infection. Diagnosis is by isolation from peripheral blood monocytes. Treatment is with ganciclovir or foscarnet as there is resistance to acyclovir. Respiratory syncytial virus manifests as an upper respiratory infection, which soon progresses to involve the lower respiratory tract. It has a high mortality and can be treated with ribavarin with or without intravenous immunoglobulin that needs to be given before the pneumonia develops. Influenza, too, has a similar clinical course (upper respiratory tract involvement initially progressing to lower respiratory tract disease) and a high mortality. The course may be complicated by secondary bacterial, viral and fungal infections.
Returning to the case being discussed, the diagnosis, which fits best, is Strongyloides stercoralis infestation. S. stercoralis infection is acquired before SOT and has minimal symptoms. Larvae from faecally contaminated soil penetrate the skin or mucosa, are carried by the blood stream to the lungs, break into the alveoli, ascend, are swallowed and reach the small intestine. Adult female worms produce eggs by parthenogenesis. These eggs hatch locally, producing rhabditiform larvae that are then converted to infectious filariform larvae. These larvae penetrate the colonic mucosa or perianal skin to enter the blood stream. This unusual ability to replicate in the human host produces the autoinfection cycle, which can persist for decades without further exposure. This is held in check by unknown components of the immune system. As immunity wanes, especially due to steroids, autoinfection accelerates leading to increasing numbers of infectious filariform larvae producing the hyperinfection syndrome. Enterocolitis, lung involvement (interstitial, alveolar, miliary pattern), hematogenous spread to the heart, skin, central nervous system, kidney, liver and secondary invasive bacteremia may characterize this state. Eosinophilia is common in the immunocompetent patient, but may be seen in only 33% of the immunocompromised hosts. Raised IgE levels, skin rash, wheezing prompt the clinician to increase the steroid dose, which makes matters worse. A high mortality of about 80% is encountered among SOT recipients, despite treatment. The diagnosis can be made by demonstrating filariform larvae in stools and in samples from sites of potential larval migration. Multiple (warm) stool samples are examined for filariform larvae. Eggs are not detectable. Duodenal aspirate, jejunal biopsy, sputum, BAL fluid and lung biopsy are the other fluids/specimens that may be examined. Thiabendazole 25mg/kg twice a day for a period of 2-3 weeks remains the drug of choice. Ivermectin 200 mg/kg can also be used. All potential SOT recipients require evaluation and if infection is present, they require treatment. Thus, my diagnosis is Hyperinfection syndrome of Strongyloides stercoralis with enterocolitis, lung involvement and a secondary bacterial sepsis syndrome, which can explain all the features, and there is nothing against it. The diagnostic procedure which I would suggest would be multiple (warm) stool samples, duodenal aspirates, sputum samples, which if negative would necessitate further search. Meanwhile, empiric treatment may be started. A direct identification of the pathogen, or a tissue-based diagnosis is essential, especially for nonbacterial and non-infectious causes. With bronchoscopy and BAL, the diagnosis may still not be forthcoming in 30% of instances. A trans-bronchial biopsy (TBB) or an open lung biopsy (OLB), though an invasive procedure, is needed, and is less risky than a failed diagnostic procedures or ineffective or toxic empiric therapy.
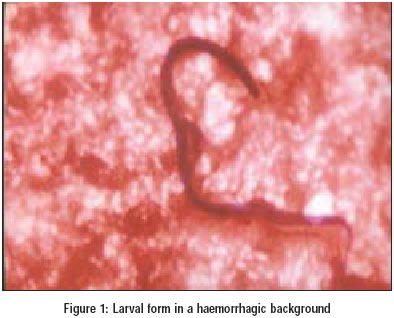
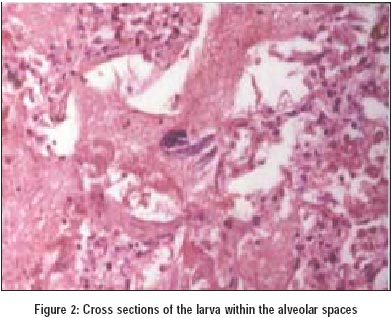
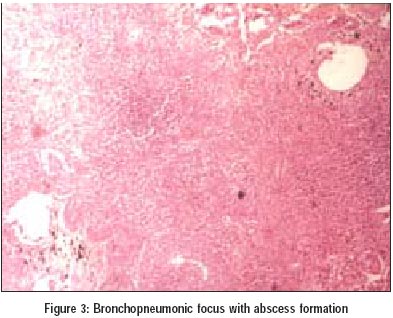
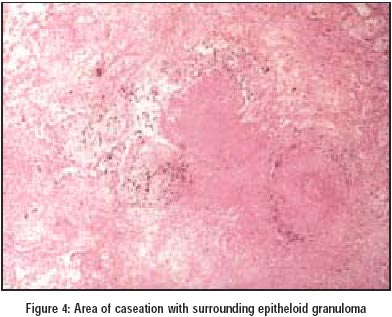
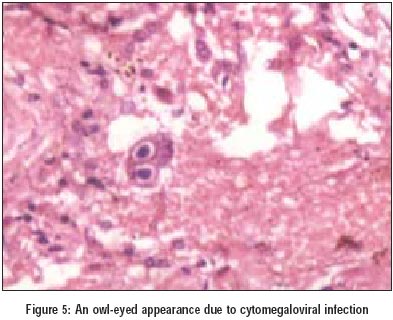
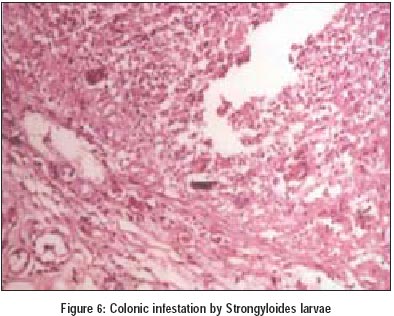
Pathological Discussion (By P. Vaideeswar) Owing to a lack of clinical response, bronchoscopy was performed and secretions aspirated. The examination of bronchial secretions revealed a few larval forms in a haemorrhagic background. The larvae were slender, spindle shaped, measuring about 250 mm in length and 20 mm in breadth, with piriform posterior bulbs and blunt tail ends, suggestive of filariform larvae of Strongyloides stercoralis (Figure 1). Despite the institution of therapy with albendazole the patient succumbed to his illness after six days. At autopsy, both the lungs were extremely firm with haemorrhagic cut surfaces. Microscopically, the alveoli were flooded with oedema fluid, red cells with thick bright pink hyaline membranes clinging to the alveolar septa and larval forms cut in different planes (Figure 2). In addition, there were foci of bronchopneumonia complicated by abscess formation, progressive tuberculosis and cytomegalovirus infection (Figures 3, 4, 5). Colonic strongyloidiasis was also present (Figure 6). Infection with S. stercoralis commences with cutaneous penetration, vascular migration and final localisation in duodenum and jejunum of the filariform larvae where it persists as an asymptomatic or symptomatic infestation.1 About 50% of the individuals especially children, the elderly and the unclean present with features of chronic infestation such as diarrhoea, abdominal pain, nausea, vomiting and weight loss. In the usual life cycle, the eggs hatch in the bowel into rhabditiform larvae, which are passed in the faeces. In moist soil, they moult to become filariform larvae. Sometimes, this transformation occurs within the mucosa of the small intestine or perianal skin leading to persistent autoinfection.1 This results in recurrent pulmonary migration consequently increasing the chances of persistent bronchial infection. The autoinfection is amplified in immunosuppressed individuals, where the parasite multiplies massively, an event known as hyper-infection with frequent dissemination to distant organs including lungs. Such an invasion might be common place with the advent of AIDS and aggressive therapy with immuno suppressants,2-5 as seen in the present case. High index of clinical suspicion and early diagnosis forms the key to successful treatment in pulmonary strongyloidiasis, as these larval forms can be picked up on routine sputum or bronchoscopic secretion examination,6 well exemplified in the present case who was a renal transplant recipient. But, it is important to differentiate these from other nematodes on the basis of external and internal characteristics.1 In the present case, apart from the lung, larvae were also seen in the colon, a rare finding. In the lungs, the larvae had induced diffuse alveolar damage, pneumonia and abscesses. In addition, the lung harboured active tuberculosis and cytomegalovirus infection. We would therefore like to stress upon the need for more vigilant search and reliance on investigations such as bronchoalveolar lavage for ruling out other opportunistic co-existing with pulmonary strongyloidiasis.
Soman R, Vaideeswar P,* Shah H,** Almeida AF** Department of Medicine, PD Hinduja National Hospital and Medical Research Centre, Mahim, and Departments of Pathology,* and Nephrology,** Seth GS Medical College and KEM Hospital, Parel, Mumbai, India.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02065f4.jpg] [jp02065f5.jpg] [jp02065f1.jpg] [jp02065t3.jpg] [jp02065f3.jpg] [jp02065t2.jpg] [jp02065f2.jpg] [jp02065t1.jpg] [jp02065f6.jpg] [jp02065t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}