 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 3, 2002 pp. 203-205 Spontaneous Aortocaval Fistula Rajmohan B The City Hospital NHS Trust, Dudley Road, Birmingham, UK. Code Number: jp02069 Abstract: Spontaneous aortocaval fistula is rare, occurring only in 4% of all ruptured abdominal aortic aneurysms. The physical signs can be missed but the presence of low back pain, palpable abdominal aortic aneurysm, machinery abdominal murmur and high-output cardiac failure unresponsive to medical treatment should raise the suspicion. Pre-operative diagnosis is crucial, as adequate preparation has to be made for the massive bleeding expected at operation. Successful treatment depends on management of perioperative haemodynamics, control of bleeding from the fistula and prevention of deep vein thrombosis and pulmonary embolism. Surgical repair of an aortocaval fistula is now standardised repair of the fistula from within the aneurysm (endoaneurysmorraphy) followed by prosthetic graft replacement of the aneurysm. A case report of a 77-year old woman, initially suspected to have unstable angina but subsequently diagnosed to have an aortocaval fistula and surgically treated successfully, is presented along with a review of literature. (J Postgrad Med 2002;48:203-205) Key Words: Aortocaval fistula, aortic aneurysm rupture, imaging, endoaneurysmorraphy, auto-transfusion, endovascular stent. Spontaneous aortocaval fistula (ACF) is found in 1 % of all operations for an abdominal aortic aneurysm (AAA) and 4% of operations for ruptured aneurysms.1 Early diagnosis and surgical treatment are necessary for a successful outcome. A case report of a 77-year old woman, initially suspected to have unstable angina but subsequently diagnosed to have an aortocaval fistula and surgically treated successfully, is presented.
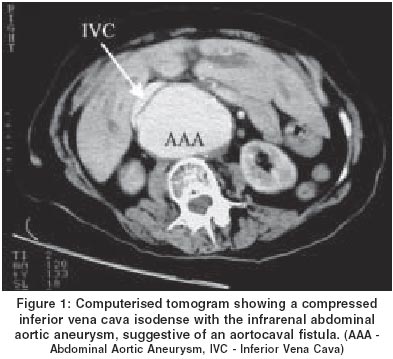
Case History A 77-year-old lady was admitted with a 4-hour history of chest pain, associated with shortness of breath and sweating. The pain was not relieved by glyceryl trinitrate (GTN) spray and was much worse than her usual angina pains. Significant medical history included transient ischaemic attacks (TIA) and angina. She smoked 15 cigarettes a day. On examination, she was in considerable discomfort. The heart rate was 94/min, blood pressure 99/34 mmHg, respiratory rate 20/min and oxygen saturation 99% on room air. Auscultation of the chest revealed coarse crepitations in the right lung base. There was a non- tender pulsatile epigastric mass, suggestive of an abdominal aortic aneurysm. An electrocardiogram (ECG) showed ST depression in leads V3 to V6, but there were no dominant R waves to suggest an acute myocardial infarction. She was admitted to the Coronary Care Unit with a clinical diagnosis of unstable angina and treated accordingly. Over the next 6 hours, her blood pressure did not improve and she complained of right hip and buttock pain. A thrill was felt on the right flank and a bruit heard on auscultation. An echocardiogram showed normal left ventricular function and normal cardiac valves. An urgent Computerised Tomogram (figure 1) showed an infra-renal abdominal aortic aneurysm 8.5 cm in transverse diameter, with early detection of contrast material in the inferior vena cava, suggestive of an aortocaval fistula. She underwent an emergency laparotomy. A trans-peritoneal approach was chosen. There was no evidence of rupture of the aortic aneurysm into the retroperitoneum or the peritoneal cavity. As the area between the aorta and the inferior vena cava was inflamed and oedematous, the aorta was exposed from the diaphragm to its bifurcation by medial visceral rotation behind the left kidney. The aorta was clamped proximally between the origins of the Coeliac and Superior mesenteric arteries and distally at the common iliac bifurcations. With the assistant ready with two swab-sticks, the aneurysm sac was opened. Bleeding from the fistula was controlled by the assistant compressing the vena cava proximal and distal to the fistula (from within the aneurysm sac), with the two swab-sticks. The fistula was oversewn from within the aneurysm sac with 3/0 prolene and the aneurysm replaced with an 18 mm gelsoft straight graft. She made a slow but uneventful postoperative recovery.
Discussion An aortocaval fistula is found in 1% of operations done for an abdominal aortic aneurysm and 4% of operations for ruptured aneurysms.1 Most abdominal aortic aneurysms rupture either into the retroperitoneum or into the peritoneal cavity. Rupture into the inferior vena cava, the duodenum, the iliac vein or the left renal vein are very rare. The original description of an aortocaval fistula is attributed to James Syme in 1831.2 Javid,3 Eisman and Hughes4 and DeBakey et al5 reported successful repairs. Prior to the production of prosthetic grafts for vascular replacement, only desperate measures such as quadruple ligation and packing were available.6 Matas, who described the technique of endoaneurysmorraphy for traumatic fistulas, significantly influenced the treatment of aortocaval fistula.7 An aortocaval fistula commonly arises from an enlarging atherosclerotic aorta. It can also result from penetrating abdominal trauma and iatrogenic trauma at lumbar disc surgery. Rare causes include mycotic aneurysm, syphilis and connective tissue disorders such as Ehlers-Danlos syndrome and Marfan's syndrome. Overwhelming majority of patients affected are males in their seventh and eighth decades of life. Because the aortocaval fistula is rare and has an elusive clinical presentation, it can be easily overlooked. Clinical presentation is commonly acute but long-standing complaints are also reported. Half the patients present with high-output, hyperdynamic circulation with a widened pulse pressure and a relatively low diastolic pressure. The triad of low back pain, a palpable abdominal aortic aneurysm and a machinery abdominal murmur/ continuous bruit is diagnostic8 and may be associated with high output cardiac failure and regional venous hypertension.9 The murmur may be absent if the fistula is partially or totally occluded by thrombus. Other physical findings include jugular venous distension, pulmonary oedema, hepatomegaly, ascites, cyanosis, haematuria, haematochezia, scrotal oedema, priapism, pulsating varicose veins and lower extremity oedema in long- standing cases. There is a striking contrast between the bluish-mottled lower extremities and the pale cold upper extremities. When the aortocaval fistula is not recognised, an attempt to treat the heart failure is unsuccessful. Preoperative diagnosis of an aortocaval fistula is helpful in planning operative strategy, in preparing for the massive blood loss and for avoiding dislodgement of atheromatous debris that can embolise across the fistula causing pulmonary embolism. An ECG may reveal a right ventricular strain pattern including T wave inversion and ST segment depression in the precordial leads and S1Q3 pattern. The imaging modality of choice for diagnosis of an aortocaval fistula is the Computerised Tomogram (CT), as it is non-invasive. CT findings include early detection of the contrast medium in the dilated inferior vena cava, which is isodense with the adjacent aorta, an associated aortic aneurysm, loss of the normal anatomic space between the aorta and vena cava and rarely one can even visualize the abnormal communication between the aorta and vena cava. Successful treatment depends on management of perioperative haemodynamics, control of bleeding from the fistula and prevention of thromboembolism. An aortocaval fistula causes a sudden diversion of blood flow from the high-resistance arterial circuit to the low-resistance and high-capacitance venous circuit. This produces a decrease in total peripheral resistance with an increase in venous resistance, venous pressure and volume. The heart rate, stroke volume, cardiac output and cardiac work are increased. The myocardium hypertrophies and then dilates, if untreated it leads to irreversible hyperdynamic cardiac failure. As blood is diverted through the fistula, arterial perfusion distal to the fistula is reduced. The raised renal venous pressure causes a decrease in the renal arterial perfusion pressure. The renin-angiotensin system is activated by the decreased distal perfusion and reduced renal arterial perfusion pressure. This leads to increase in the secretion of aldosterone, which, in turn, causes plasma expansion in an attempt to increase perfusion. A Swan-Ganz catheter or transoesophageal echocardiography will be useful in monitoring and maintaining haemodynamic stability in the peri-operative period. A Swan-Ganz catheter may also be a useful adjunct in the diagnosis as it demonstrates the presence of high cardiac index, normal or increased stroke volume, low systemic vascular resistance and abnormally high oxygen concentration in the vena cava. All the haemodynamic abnormalities are rapidly reversed with surgical closure of the fistula. Risk of excessive bleeding is one of the hazards of this surgery. An autotransfusion device can reduce or avoid external transfusion requirements. The standard surgical approach is the trans-peritoneal one. However, an extra-peritoneal approach through an incision in the 11th intercostal space in the left flank enables minimal dissection through thick fibrotic tissues prevalent in the anterior and lateral aspects of the aneurysm. In our patient, a trans-peritoneal approach was used but the aorta was exposed from the diaphragm to the bifurcation by medial visceral rotation behind the left kidney. Proximal control of the aortic aneurysm is achieved prior to distal control to avoid a sudden increase in fistula flow. Minimal manipulation or mobilization of the aorta is performed to reduce vascular injury, excessive operating time, bleeding from engorged retroperitoneal and pelvic veins and paradoxical embolization of intraluminal thrombus. The fistula is located by palpating the inferior vena cava for the characteristic thrill. It is visualised after opening the aneurysm sac and evacuating the thrombus or atheroma. Venous bleeding is controlled by direct pressure (digital or swab-stick) or balloon tipped catheters (Foley or Fogarty) inserted through the fistula into the proximal and distal IVC. Naito et al 10 have used a novel method to minimize bleeding. They inserted two Fogarty catheters in the vena cava pre-operatively through the right femoral vein. One catheter was positioned just proximal to the ACF while the other was placed just distal to ACF under angiographic guidance. The balloons were inflated after aortic clamping and before opening the aneurysm sac. Surgical intervention consists of repair of the fistula from within the aneurysm, followed by prosthetic graft replacement of the aneurysm. The fistula is primarily closed with a non-absorbable suture but patch repair with Dacron or bovine pericardium has also been reported. When the tissue did not hold sutures, Uemura et al used aortic exclusion, packing the aneurysm sac with omentum and re-establishing continuity with aorto-bifemoral synthetic graft.11 If the inferior vena cava is extensively eroded, ligation may be an option. In extreme cases, if the bleeding is uncontrolled by usual manoeuvres, total circulatory arrest with deep hypothermia minimises blood loss and permits repair. Endovascular stenting and exclusion of the aneurysm is possible if the anatomy of the aneurysm permits such a procedure.12 Unlike for a free or even a contained AAA rupture, emergency repair of an ACF may not always be necessary, allowing time to obtain a suitable endograft. Endovascular stenting averts the significant blood loss encountered in the conventional surgical repair. Another concern is the possibility of thromboembolism. The incidence of deep vein thrombosis is up to 20% after surgical repair and thromboprophylaxis is necessary. Manipulation of the aneurysm prior to cross clamping can result in embolisation of mural thrombus. Fogarty balloons10 and extra-caval clip can reduce chances of pulmonary embolism. Operative mortality of the aortocaval fistula is about 30% and appears to be no greater than that seen with ruptured abdominal aortic aneurysms in general.13 The mortality and morbidity relate to the degree of acute blood loss, myocardial infarction, coagulopathy and renal failure.
Acknowledgement Author thanks Mr. S. Silverman, Consultant Vascular Surgeon, The City Hospital, Birmingham, for helping in the preparation of this report and Mrs. Priya Rajmohan for the technical help in preparing the manuscript.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02069f1.jpg] |
| |||||||||

{kind=link}