 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 3, 2002 pp. 213-214 Intradiploic Epidermoid Cyst Narlawar RS, Nagar A, Hira P, Raut AA Department of Radiology, Seth G. S. Medical College and K.E.M. Hospital, Parel,
Mumbai - 400012, India. Code Number: jp02073
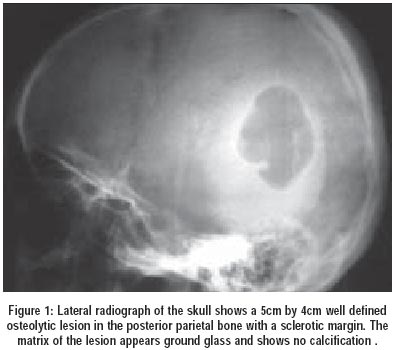
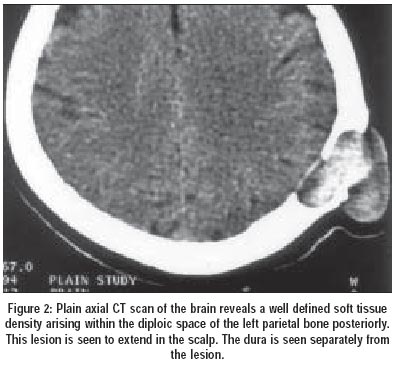
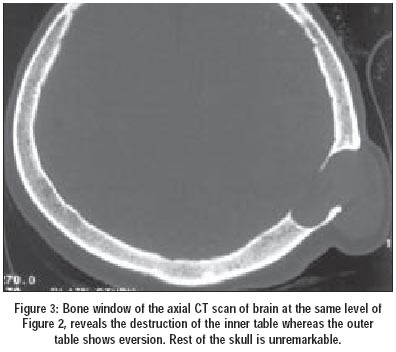
A 35-year-old lady, presented with approximately 5 cm X 4 cm sized swelling in the left parietal region since childhood. There was history of progressive increase in the size of the swelling since childhood. There was no history of trauma. There was history of pain associated with swelling since last two months. On examination, the swelling was soft, non-tender and could be moved over the underlying bone. The skin over the swelling could not be retracted. Frontal and lateral radiograph of the skull showed an approximately 5 cm X 4 cm , well defined osteolytic lesion in the left posterior parietal bone (Figure 1). The inner table was scalloped and the outer table was everted (Figure 2). There was no evidence of calcification or periosteal reaction. Rest of the skull was unremarkable. For better delineation of the lesion, plain and contrast enhanced axial computed tomographic (CT) scan was performed. Plain CT scan revealed, a 5 cm sized soft tissue density lesion seen within the diploic space of the left posterior occipital bone with attenuation values ranging between 20 Hounsfield unit (HU) to +20 HU (Figure 3). This lesion was seen to protrude outside the margins of the skull and the dura matter was seen separately from the lesion. There was no calcification within the mass. On contrast there was no appreciable enhancement. Rest of the cerebral parenchyma was normal. Under general anaesthesia, left posterior occipital linear incision was taken and total removal of the cyst was performed. On cross-section the tumour was pearly white and smooth, containing a lamellar keratinised debri. The microscopic examination revealed the cyst to be lined by stratified squamous keratinised epithelium. There were no areas of calcification or haemorrhage. The post-operative course of the patient in the ward was uneventful and patient was discharged on 3rd post-operative day.
Discussion Epidermoid tumours account for less than 1% of the cranial tumors. 75% of which are located intradurally and 25% are located within the diploic spaces. Intradiploic epidermoid cysts are insidious lesions. They most commonly present in the third or fourth decade of life as a long-standing painless subcutaneous scalp swelling covered with normal skin.1 Most epidermoid cysts are thought to result from a displacement of ectodermal tissue during the third to fifth week of embryogenesis. 2 Bony epidermoid cysts are mainly located in the skull, although other locations, including the mandible, maxilla, temporo-mandibular joint, distal phalanges, tibia and femur, have been described.3 A minority of cranial epidermoids arise secondary to trauma and are associated with implantation of epidermal cells into the skull. This mechanism is more common in the spine in relation to the lumbar vertebra. The most common presentation of the calvarial intradiploic epidermoid is a long-standing, asymptomatic lump on the head. Headache and focal tenderness may be present. Rarely, large lesions may be associated with focal neurological signs. Superinfection or bleeding has been described. Malignant transformation, intracranial hypertension, seizures and focal neurologic signs have been described in patients with large cysts.4 Diagnosis of epidermoid cysts can be challenging. On plain films and CT scan, there is a well-defined lytic lesion centered in the diploic space with or without sclerotic margins. Both inner and outer tables are involved, as in our case. The lesion typically shows the density ranging between 20 to + 20 HU. Magnetic resonance imaging reveals varying signal intensity for T1-weighted images (high signal intensity being associated with hemorrhagic fluid in the cyst). These cysts are consistently hyperintense on T2-weighted images. Occasionally, high signal can be seen on T1-WI from hemorrhagic or proteinaceous fluid. No contrast enhancement is present unless the lesion is super-infected. Surgical excision of the cyst is performed for diagnosis, to relieve any symptoms, for cosmetic improvement and to avoid potential complications, including intracranial mass effect, abscess formation, bleeding, and malignant change. Ideally, surgery is performed, with the goal being total removal of the capsule, which must be dissected carefully from the bone and dura mater. 5 Dermoid cyst, cavernous haemangioma, eosinophilic granuloma, and giant cell reparative granuloma are the commonest radiological differential diagnoses. Dermoid cysts are typically associated with the suture lines, commonly occur in orbital region and in the midline, usually present in childhood, often contain fat. Eosinophilic granulomas are less heterogeneous, are often tender and have "beveled edge" appearance. Cavernous hemangiomas have honeycomb or radiating sunburst appearance. Giant cell reparative granulomas are lytic lesions without sclerosis and on MRI are iso-intense to gray matter and enhance intensely after gadolinium. Occasionally, hemorrhagic fluid or calcification is noted. Rarely, these cysts may undergo malignant degeneration. 6 After diagnosis and complete excision, careful follow-up is essential, as recurrence rates of 8.3% to 25.0% have been reported.7 In conclusion, there is a wide variety of lesions that may present as solitary calvarial lesions. 35 to 40 % of them will have intracranial extension, hence imaging is essential prior to any surgical intervention. The present case illustrates a common presentation of a relatively uncommon tumor of the cranium. Intradiploic epidermoid cysts are an important diagnosis to consider in a patient who presents with a slowly progressive scalp mass. The prognosis is generally good with appropriate surgical intervention.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02073f2.jpg] [jp02073f1.jpg] [jp02073f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}