 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 3, 2002 pp. 226-231 The Role and Effectiveness of Adjunctive Hyperbaric Oxygen Therapy in the Management of Musculoskeletal Disorders Wang J, Li F, Calhoun JH, Mader JT Department of Orthopaedics and Rehabilitation, University of Texas Medical
Branch, Galveston, TX, USA. Code Number: jp02077
Abstract: The management of musculoskeletal disorders is an increasing challenge to clinicians. Successful treatment relies on a wide range of multidisciplinary interventions. Adjunctive hyperbaric oxygen (HBO) therapy has been used as an orthopaedic treatment for several decades. Positive outcomes have been reported by many authors for orthopaedic infections, wound healing, delayed union and non-union of fractures, acute traumatic ischaemia of the extremities, compromised grafts, and burn injuries. Severe side effects have also been reported with this therapy. To aid in the use of HBO therapy in orthopaedics, we reviewed 43 papers published in the past four decades and summarised the mechanisms, effectiveness, indications and contraindications, side effects, and cost impact of adjunctive hyperbaric oxygen therapy in the management of difficult musculoskeletal disorders. Adjunctive HBO therapy is an effective treatment modality for the management of some severe and refractory musculoskeletal problems. If appropriate candidates are carefully identified, hyperbaric oxygen is a limb- and sometimes life-saving therapy. HBO therapy significantly reduces the length of the patient's hospital stay, amputation rate, and wound care expenses. Thus, it is a cost-effective modality. A clinician must understand the side effects and risks of HBO treatment. Close monitoring throughout the treatment is warranted to minimise the risk to the patients. (J Postgrad Med 2002;48:226-231) Key Words: Hyperbaric oxygen, musculoskeletal disorders, osteomyelitis, wound care, cost/benefit analysis
Many musculoskeletal disorders, such as refractory osteomyelitis, diabetic foot ulcers, non-union of fractures, severe soft tissue infections, and compromised grafts, are difficult to manage. They require multidisciplinary treatment. Great efforts have been taken in the past few decades to improve the management of such cases with advanced antibiotics, debridement, modern orthopaedic devices, and aggressive wound care. The outcome however, has not been optimal. Hyperbaric oxygen (HBO) therapy, in adjunct with the above treatment modalities, has shown to be of great benefit in the management of these hard-to-treat problems. It reduces the morbidity and mortality of these musculoskeletal diseases, as well as the cost of the care. Like any other treatment method, HBO therapy can also cause severe side effects and has associated risks. To understand more about this therapeutic modality, we reviewed forty-three papers published in the past four decades to clarify the mechanism, indications and contraindications, effectiveness, side effects, risks, and cost impact of HBO therapy.
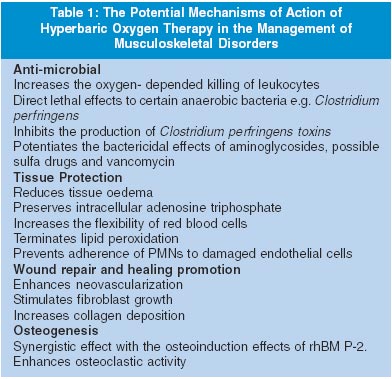
Principles and Mechanisms of Hyperbaric Oxygen Therapy The blood transports oxygen in two different ways: chemically, bound to haemoglobin in erythrocytes, and physically, dissolved in plasma according to Henry's law.1 At normal atmospheric pressure, the oxygen in the arterial blood is almost entirely bound to haemoglobin; however, while breathing 100% oxygen at two or three atmospheres absolute (ATA), a significant proportion of the arterial oxygen is in dissolved form. An increased PO2 has a negligible impact on total haemoglobin oxygen content, but it does result in an increase in the amount of oxygen dissolved directly into plasma. HBO therapy is defined as a mode of medical treatment in which the patient is breathing 100% oxygen intermittently at a pressure greater than one atmosphere. Treatment can be carried out in either a monoplace or multiplace chamber. The monoplace chamber accommodates a single patient and the entire chamber is pressurized with 100% oxygen. The multiplace chamber holds two or more people (patients and support personnel). The multiplace chamber is pressurised with compressed air while the patients breathe 100% oxygen via masks, or head tents. The potential mechanisms of HBO therapy are listed in Table 1.
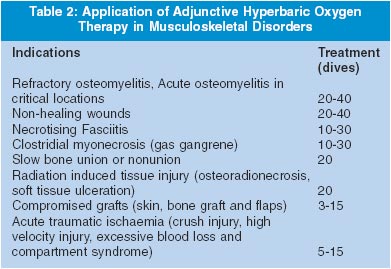
HBO Therapy in the Orthopaedic Disorders HBO therapy was designed for and initially used to treat patients involved in diving accidents or with decompression sickness. However, its indications have increased over the past few decades. Currently, there are twelve indications for HBO therapy approved by the Undersea and Hyperbaric Medical Society (UHMS) in the United States.2 There are, however, over a hundred indications internationally, although most of them have not been proven by controlled studies.2 In the field of orthopaedics, HBO alone or as adjunctive therapy has proved useful in the management of refractory osteomyelitis, non-healing wounds (diabetic foot ulcers and chronic ulcers from chronic limb ischemia), and acute osteomyelitis in critical locations such as the skull or sternum.3 HBO is also indicated in delayed union or non-union of fractures, radiation-induced tissue injury (osteoradionecrosis, soft tissue ulceration, and fibrosis), thermal burns, and acute traumatic ischaemia (crush injury, high velocity injury, excessive blood loss, and compartment syndrome). Finally, compromised grafts (skin and bone grafts and muscle flaps) are also frequently treated with hyperbaric oxygen (Table 2). These clinical indications were evaluated in a Consensus Conference by the UHMS that classified the application of HBO therapy according to its efficacy; indications were classified as strongly recommended, recommended, and optional. In a clinical setting, each patient with the above indications is carefully evaluated individually as a candidate for HBO therapy. Other factors including the patient's condition, comorbidity, past medical history, and current medications are considered for the selection of candidates. The Cierny-Mader classification system for example, is currently used as a guide to determine candidates for adjunctive HBO therapy for osteomyelitis.4 In this system, osteomyelitis is classified in four stages: stage I (medullary), stage II (superficial), stage III (localised), and stage IV (diffuse). The patient's host status is also included in this classification. Patients are classified as a normal host (A), compromised host (B), or if the treatment is worse than the disease (C). Appropriate candidates for HBO treatment fall in class IIIB and IVB.5,6
Hyperbaric Oxygen as Adjunctive Therapy for Osteomyelitis HBO has been used for refractory osteomyelitis as an adjunctive therapy by many authors.2-4,6-13 Standard treatment for osteomyelitis includes radical local debridement, local antibiotic beads, and systemic antibiotics.4,7-9 Bone grafts are performed secondarily to fill in bony defects. The term refractory osteomyelitis is applied to bone infections that fail to respond despite adequate surgical and antibiotic therapy. Systemic host and local immunocompromised factors are frequently associated with refractory osteomyelitis.4Long-term antibiotic therapy and multiple surgeries are often required. Failure of treatment or recurrence of osteomyelitis often leads to amputation. In addition, long-term antibiotic therapy is associated with potential severe adverse effects to several organs and invasive surgery with multiple complications. Hyperbaric oxygen can be used as an adjunctive treatment in chronic refractory osteomyelitis along with culture-directed antibiotics, surgical debridement, and nutritional support. The results of multiple clinical studies have suggested a beneficial effect with the addition of adjunctive hyperbaric oxygen therapy to conventional treatment regimens for osteomyelitis in terms of reduced hospital stay and amputation rates,10,11 whereas other clinical studies12 have failed to demonstrate such a benefit. The following are the mechanisms of action of HBO therapy in the treatment of osteomyelitis: Firstly, HBO enhances oxygen-dependent leukocyte killing through the production of hydrogen peroxide and superoxide by providing increased oxygen tension in the hypoxic tissue. In earlier animal studies, the oxygen tension of infected bone increased from 23 mmHg to 104 mmHg in response to HBO at 2 ATA.14 Since the bactericidal activity of leukocytes in vitro is directly related to local oxygen tension, transient reversal of hypoxia might increase clearance of bacteria.15 Secondly, optimal tissue oxygen tension enhances osteogenesis16,17 and neovascularization18 to fill the dead space with new bone and soft tissues. HBO has also been shown to enhance osteoaclastic activity5 to remove bony debris. Synergistic effects of HBO on bone healing with bone morphogenic protein (BMP) were also demonstrated.19 Finally, HBO has also been shown to potentiate the antimicrobial effects of aminoglycosides, and possibly sulpha drugs and vancomycin, in the killing of susceptible bacteria.9 Patients with osteomyelitis are usually treated at 2.0 to 2.5 ATA for 90-120 minutes per day and typically receive 20-40 treatments. Regrettably, there have been no randomised, prospective, double blind studies of HBO therapy in patients with chronic refractory osteomyelitis. Many clinical variables involved in osteomyelitis exist, which make clinical studies difficult to design and evaluate. These variables include different infected bone sites, organisms, and antibiotics. Additional variables include type, adequacy, and timing of surgical debridement, dead space management, the status of adjacent soft tissue, the routes and duration of antibiotic(s) treatment, and the amount of bone penetration by the antibiotic(s). More clinical research is needed to address the effectiveness of HBO therapy, despite the problems in research designs inherent in the osteomyelitis population.
Hyperbaric Oxygen Therapy in Non-Healing Wounds Wounds that fail to respond to established medical and surgical management are the most frequent entity treated with HBO therapy in United States. These wounds usually develop in compromised hosts with multiple local and systemic factors contributing to impairment of tissue repair. These include diabetic foot ulcers, non-healing traumatic wounds, and peripheral vascular insufficiency ulcers. Transcutaneous oxygen tension assessment of the involved extremity may help to identify the appropriate candidates for HBO by documenting low oxygen tension in the area of the ulcer. Patients are generally treated at 2.0 to 2.5 ATA for 90-120 minutes per day and receive 20-30 treatments. The heterogeneity of diabetic foot ulcers contributes to the confusing role of HBO as a treatment modality. Neuropathic foot ulcers with adequate blood supply can be healed with appropriate wound care and off-loading. Patients with non-healing ischemic ulcers with vascular lesions not amenable to angioplasty or vascular surgery may benefit from HBO therapy. In a hypoxic environment, wound healing is halted by decreased collagen production, poor capillary angiogenesis, and impaired oxygen-dependent intracellular leukocyte killing. HBO therapy promotes neovascularisation18 and increases endothelial cells, fibroblast proliferation20 and collagen deposition.21 In addition, HBO can modify the cellular functions of the activated neutrophil, resulting in increased oxidative microbial killing and decreased neutrophil-endothelial adhesion.15 At the molecular level, a recent study showed that HBO up-regulates platelet-derived growth factor receptor messenger RNA activity22 and the synergistic effect with growth factor23 has also been demonstrated. All of these modifications may contribute to changing a non-healing wound status to active wound healing. Multiple anecdotal reports and retrospective studies on HBO therapy in diabetic patients suggest that HBO can be an effective adjunct in the management of diabetic wounds. Prospective studies also show the beneficial effects of HBO therapy as adjunctive treatment of the ischaemic foot ulcer. Of the seven published studies pertaining to the diabetic foot, three of them were randomised, controlled clinical trials. In one of the prospective, randomised, controlled studies, Faglia and colleagues24 report significantly fewer major amputations among patients with Wagner grade IV lesions in the HBO group compared with patients in the control group. There was no statistical difference in minor amputations between the HBO and control groups, nor was there any difference in major amputation rates among the less severe Wagner ulcer classification groups. The second prospective, randomised, controlled study reported significantly fewer major amputations in the HBO group than in the standard treatment control group25 however, there was no difference in the length of hospitalisation or the number of minor amputations between the groups. In the third prospective, randomised, controlled study, Kalani et al26 did a long-term (three years) follow up of wound healing and amputation rates in 38 patients with diabetic foot ulcers. The patients were randomly divided into two groups, HBO and conventional treatment. Patients in these two groups were matched for age, gender, duration of diabetes, blood pressure, TCPO2, and HbA1C. They found that the wound-healing rate was 76% in the group with HBO therapy and 48% in the group without HBO therapy. The amputation rate was 12% in the HBO therapy-group and 33% in the group not given HBO therapy. The Fourth Consensus Conference of the European Committee in Hyperbaric Medicine concluded "further controlled studies should be carried out to obtain more precise data on HBO before widely implementing this therapy in patients with diabetes."27 In the clinical setting, HBO treatment is considered in patients with Wagner grade III-V lesions that do not respond to conventional treatment.
Necrotising Fasciitis Necrotising fasciitis is a severe, fulminant infection most commonly encountered in patients with diabetes mellitus, cirrhosis, and intravenous drug abuse. The infection can spread, unrecognised, along fascial planes beneath seemingly normal skin. The relatively benign appearance of the extremity is misleading and often results in a delay in diagnosis and increases morbidity or death. Necrotising fasciitis is a rapidly progressing synergistic bacterial infection with a high mortality rate. Immediate aggressive surgical debridement in combination with antibiotic therapy is necessary for control of these limb- and life-threatening, soft-tissue infections. HBO therapy is frequently used as adjunctive therapy in the management of necrotizing fasciitis. Patients generally receive 5 to 30 sittings of HBO at 2.0 to 2.5 ATA for 90 to 120 minutes. Although there are no randomised trials of HBO in these infections, clinical reports28-30 and meta-analysis of clinical case reports31strongly support the use of HBO therapy.
Gas Gangrene Gas gangrene, or clostridial myonecrosis, is commonly encountered in those extremity-wounds that involve devitalised or necrotic soft tissues.32 Infection with Clostridium perfringens in devitalised tissue is the most common cause. Clostridial microorganisms are anaerobes that produce local and systemic toxins. Wide surgical debridement and appropriate antibiotic therapy remain the standard treatment modality. HBO therapy induces high oxygen partial pressure in all tissues; achievable tissue oxygen levels are lethal to some obligate anaerobic bacteria such as Clostridium perfringens.33 HBO therapy also has an anti-oedema effect, causes activation of fibroblasts and macrophages, and stimulates angiogenesis. In animal models, the addition of HBO therapy to standard management has been shown to have a synergistic effect in reducing morbidity and mortality.34 Although no prospective human studies are available, retrospective data indicate that concomitant hyperbaric oxygen therapy has resulted in a two-fold reduction in mortality.35-37
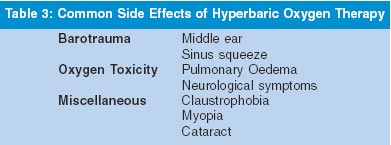
Side Effects and Contraindications of Hyperbaric Oxygen Therapy HBO therapy is generally safe and well-tolerated. Table 3 lists the most common side effects associated with HBO therapy. Most side effects are mild and reversible, but some severe consequences can occur in rare cases.38-40 Middle ear barotrauma is the most common side effect of hyperbaric therapy. It is preventable in most patients by teaching auto inflation techniques, or by using tympanostomy tubes or myringotomy for those who cannot auto inflate their middle ear compartment. Sinus squeeze occurs less frequently than middle ear barotrauma and usually occurs in patients with upper respiratory tract infections or allergic rhinitis. Claustrophobia is present in about 2% of the general population, which may cause some degree of confinement- anxiety inside the hyperbaric chamber. Mild sedation is often required for these patients in order to continue with daily hyperbaric oxygen treatment. Pulmonary and neurological manifestations of oxygen toxicity are often cited as major concerns. Seizure is rare, but has potentially severe consequences. Weaver et al reported three cases of pulmonary oedema with HBO therapy with one fatality.41 They concluded that HBO therapy may contribute to pulmonary oedema by increasing left ventricular (LV) after load increasing LV filling pressures, increasing oxidative myocardial stress, and decreasing LV compliance. HBO therapy may also alter the cardiac output between the right and left hearts; may induce bradycardia with concomitant LV dysfunction; may increase pulmonary capillary permeability and cause pulmonary oxygen toxicity. They advise caution with the use of HBO therapy in patients with heart failure or in patients with reduced cardiac ejection fraction. Absolute contraindications to HBO therapy include untreated pneumothorax and concurrent therapy with doxorubicin, cisplantin, and disulfiram. High fever, low seizure- threshold, emphysema, and upper respiratory infections are considered relative contraindications to HBO therapy.
Cost Impact The costs associated with HBO therapy have not been well-addressed in the literature. There are few publications documenting the cost-benefit analysis of this therapy. We found only two papers in the past ten years that described the cost-effectiveness of HBO treatment. Boykin et al successfully treated a case of soft tissue radiation necrosis with adjunctive HBO.42 In this example, a reduction in patient charges of greater than 30% was achieved as compared to traditional management. Cianci et al also described a significant reduction in expenses in the treatment of thermal- burn patients with adjunctive HBO therapy.43 They divided the patients into two groups; one with and another without HBO therapy. The group that received HBO therapy had an average 14.8-day decrease in length of hospital stay, a 39% reduction of surgical procedures, and an average saving of $31,600 per patient.
Conclusion HBO therapy has proven beneficial effects for several musculoskeletal disorders. Although clinical studies and trials demonstrate the overall effectiveness of HBO therapy, more clinical research and better controlled trials are needed to delineate and define the clinical effectiveness and benefits of HBO therapy in each disease entity. HBO therapy should be used in conjunction with an aggressive, multidisciplinary treatment protocol and should be considered as an adjunct to, not as a substitute for, other therapeutic procedures. It may also improve the cost- effectiveness of treatment for difficult musculoskeletal disorders.
Acknowledgements The authors would like to gratefully acknowledge the editorial assistance of Kristi Overgaard in the preparation of this manuscript.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02077t1.jpg] [jp02077t3.jpg] [jp02077t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}