 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 48, Issue 4, 2002 pp. 280-282 Evaluation of Low Dose Acth Stimulation Test in Suspected Secondary Adrenocortical Insufficiency Gandhi PG, Shah NS, Khandelwal AG, *Chauhan P, Menon PS Departments of Endocrinology, Seth G. S. Medical College and K. E. M. Hospital,
and *PD Hinduja Hospital, Mumbai, India. Code Number: jp02094 Abstract: BACKGROUND: Several studies in the last few years have shown that the standard 250µg dose used in ACTH stimulation test may be very high and have suggested that a dose of 1µg may be sufficient for evaluating hypothalamo-pituitary adrenal (HPA) axis. AIMS: To evaluate the role of low dose ACTH stimulation test in patients with suspected Secondary Adrenal Insufficiency (SAI). SUBJECTS AND METHODS: Thirty-one patients of suspected SAI with a documented pituitary lesion and seven normal healthy controls were included in the study. All the subjects underwent ACTH stimulation test with standard high dose (HD= 250 µg) and low dose (LD= 1µg) ACTH. Insulin Induced Hypoglycaemia (IIH) test was done in 7 out of 9 patients in whom the results of the two tests were discordant. The cut off for normal HD stimulation test was taken as peak cortisol response > 18 µg/dl and for LD test, either a cortisol response of > 18 µg/dl or an increment of more than 7 µg/dl over the basal value at any time during the test, on the basis of response observed in controls. RESULTS: 22/31 patients (74%) in SAI group showed concordant results with both tests, whereas nine patients had discordant results. These nine patients showed AI with LD ACTH, but HD ACTH test showed a normal response. In 7 of these 9 patients who underwent IIH, AI was confirmed in 6. CONCLUSION: The LD ACTH stimulation test seems to be better than HD ACTH stimulation test for evaluating HPA axis in patients with suspected SAI. When basal cortisol is normal, LD ACTH stimulation test detects subtle SAI. (J Postgrad Med 2002;48:280-282) Key Words: Secondary adrenal insufficiency, ACTH test, Insulin induced hypoglycaemia test Related Editorial - jp02088
Standard ACTH stimulation test using 250 mg of synthetic ACTH is the most widely used diagnostic test for the detection of secondary adrenocortical insufficiency (SAI). An area in which there is ongoing controversy is whether this accurately predicts the ability to respond adequately to stress such as major surgery. This is because occasional patients have normal response to HD ACTH stimulation test but subnormal response to Insulin Induced Hypoglycaemia (IIH) test,1,2,3 a test considered as the gold standard test for the evaluation of HPA axis.4,5,6,7 The pharmacological dose of 250 mg is useful to assess the maximum secretory capacity of the adrenal cortex. However, this dose may be excessive for the assessment of "sub clinical hypocortisolism".8 The LD ACTH stimulation test has been shown correlate well with IIH.8 A number of centres are already using the LD ACTH stimulation test. The high sensitivity and specifity of LD test in the diagnosis of mild forms of primary adrenal insufficiency is already known.9 The aim of the present study was to evaluate LD ACTH stimulation test in patients with suspected SAI and compare it with standard HD ACTH stimulation test. IIH was used as the gold standard test in all those with discordant results, for establishing diagnosis and outcome.
Patients and Methods Thirty-one consecutive cases of suspected SAI with documented pituitary lesion and 7 normal healthy controls were studied. Low dose (1 µg) ACTH aliquots were prepared from 1 vial of 250 µg Synacthen (Beta 1-24 Corticotrophin, Ciba Geigy, Mumbai, India) after diluting it in sterile normal saline solution. Aliquots were put into gamma irradiated sterile plastic tubes and kept in laboratory deep freezer at -200C. The stability of one randomly selected aliquot was tested before and after completion of the study to know the exact concentration of ACTH. At the beginning of the study 100% recovery was obtained from the sample, however at the end of the study 64% recovery was obtained i.e. the solution of 1 µg ACTH contained only 0.64 µg of ACTH. Hence, the concentration of ACTH in the aliquot for LD ACTH stimulation test during the study was between 0.64-1 µg. For short HD ACTH test, 250 µg Synacthen was used. The study was done after obtaining permission from the institutional Ethics committee. After obtaining a written informed consent HD, LD ACTH stimulation tests and IIH test were done as per the standard protocols described1 on two different days and results analysed. If the results of the two tests were discordant we used IIH as gold standard for establishing the diagnosis. The serum was separated and preserved in deep freezer at -200 in the laboratory until analysis. Plasma cortisol concentration was determined by a solid phase radioimmunoassay using a DSL (Texas, USA) kit (intra assay and inter assay variation of 1.00% and 1.5% respectively). The study was carried out over a period of one year.
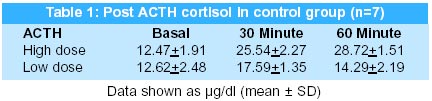
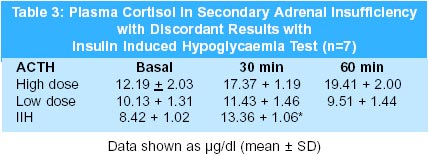
Results The patient group included 31 cases of suspected SAI (16 males and 15 females aged 33.58 + 2.17 yrs) with pituitary lesion (Pituitary tumours operated 25; Sheehan's syndrome 3; Pan hypituitarism 2 and Post Radiotherapy 1). Table 1 shows the mean peak cortisol response to HD and LD ACTH stimulation test of the controls. The peak plasma cortisol response to HD test in control subjects was seen at 60 min. (28.72 + 1.51 µg/dl), whereas the peak cortisol response to LD ACTH was seen at 30 min. (17.59 + 1.35 µg/dl). The peak cortisol response to LD ACTH seen at 30 minutes and was much lower than that of HD ACTH at 30 min. With HD ACTH, peak cortisol response of > 18 µg/dl was seen in all subjects. In the control group, peak cortisol response of > 18 µg/dl to LD ACTH was seen in 3 subjects and an increment of > 7µg/dl from the basal value was seen in the remaining 4 subjects. As these were clinically normal individuals, without any endocrine disorder, we are unable to explain the lower response in them. In view of these results, in this study, the cut off for normal HD ACTH stimulation test and IIH was taken as >18 µg/dl. For LD ACTH stimulation test, normal cortisol response was taken as either peak cortisol response of > 18 µg/dl or an increment of >7 µg/dl over the basal value at any time during the test. Out of 31 patients with SAI group, results of both ACTH stimulation tests were suggestive of AI in 16 and normal in 6 patients (concordant group). In the remaining 9 patients, HD ACTH stimulation test was normal but LD test was suggestive of AI. (discordant group) (Table 2). The basal cortisol was not different during the two days of testing in these 9 patients. The basal cortisol values in concordant group were much lower than the discordant group (Table 2). IIH test could be done in only 7 out of these 9 patients as the rest 2 patients did not give consent. In 6 out of 7 patients results of IIH confirmed the presence of AI (Table 3).
Discussion HD ACTH stimulation test is an accepted method of assessing HPA axis function. The normal range of cortisol and ACTH levels is broad and an individual can have primary or secondary AI but maintain normal basal ACTH and cortisol secretion1. Dickstein et al10 studied the response to LD ACTH in patients with chronic ACTH deficiency due to long-term glucocorticoid therapy for the first time in 1991. They concluded that 1µg ACTH causes maximal response at 30 min and it is more sensitive than HD ACTH test for the detection of early AI. Our 4 normal healthy controls did not show peak cortisol of more than 18 µg/dl. But, all these 4 subjects showed a rise of over 7 µg/dl following LD, a criterion described by Crowley et al11 for LD ACTH test. This was the rationale for accepting 7µg/dl rise after LD ACTH test as normal for this study. The peak cortisol response in the control group with HD ACTH was seen at 60 minute, and with LD ACTH at 30 minute, as seen in other studies.8,10,11 Twenty-two out of thirty one (70%) patients showed concordant results with both the tests (22 with AI and 6 normal). Although the peak cortisol response with both the tests was suggestive of AI, there was almost no increment in the cortisol response with LD ACTH whereas some increment in the cortisol response was seen with HD ACTH. This suggests that pharmacological doses of ACTH (HD) can cause some stimulation of the involuted adrenal gland, but lower and nearer physiological doses do not. Nine patients in the suspected SAI group had discordant results with LD and HD ACTH stimulation tests in our study. In the seven patients who underwent IIH test in view of discordant, presence of SAI was confirmed in 6 and in 1, it was normal (23.7 µg/dl). Hence, false positive results can be seen even with LD ACTH test in patients with normal HPA axis. Although in our patient normal HPA reserve was demonstrated by IIH test, it should be kept in mind that this patient had pituitary disease and was not a normal subject. It is thus conceivable that in this patient the LD ACTH test may have uncovered a subtle insufficiency of HPA axis. However, the definite clinical significance of this finding, if any, is still uncertain. It is interesting to note that the basal cortisol values in patients with suspected SAI showing poor response to both LD and HD ACTH were between 4 to 6 µg/dl (mean 5.66 + 0.99 µg/dl) which is low enough to diagnose AI. However, in all the 9 patients with discordant response, the basal cortisol level exceeded 10 µg/dl (a value equal to that in controls). It suggests a failing but not absent ACTH secretion that maintains basal cortisol secretion and normal response to HD ACTH in patients with discordant group. Hence our study and other studies5,8,10,12 suggest that for early detection of chronic ACTH deficiency with normal basal cortisol levels, the LD ACTH test is more sensitive and reliable than standard HD ACTH test. In our study, patient with pituitary disease (n=9) had higher number of false negative results with HD ACTH, as also demonstrated by other studies.2,4,13,14,15,16 In a review Thaler et al has concluded that the sensitivity and specificity of low dose ACTH stimulation test is higher than that of HDT when compared with IIH.17 In these patients, HPA axis dysfunction can be detected by LD ACTH test or IIH test. On the basis of above results it can be concluded that LD ACTH test is superior to HD ACTH test in detecting early ACTH deficiency especially when basal levels are normal or low normal. A larger sample size including a larger control group would be useful to confirm the results. We also feel that the standard ACTH test using 250 µg should be ideally replaced by one µg test as suggested by Tordjman18 and Beishuizen.19 The commercial availability of 1µg preparation will be helpful in this regard.
Acknowledgement The authors sincerely thank Mrs. Anjana Karavat, Senior Scientific Officer, for performing cortisol assays for this study.
References
This article is also available in full-text from http://www.jpgmonline.com/ © Copyright 2002 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp02094t3.jpg] [jp02094t2.jpg] [jp02094t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}