 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 49, No. 1, Jan-March, 2003, pp. 50-54 Symposium Cutaneous Leishmaniasis: An OverviewHepburn NC Lincoln County Hospital, Lincoln LN2 5QY, United Kingdom.
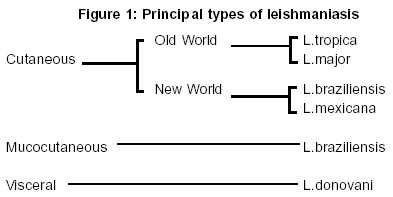
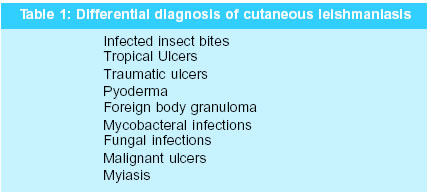
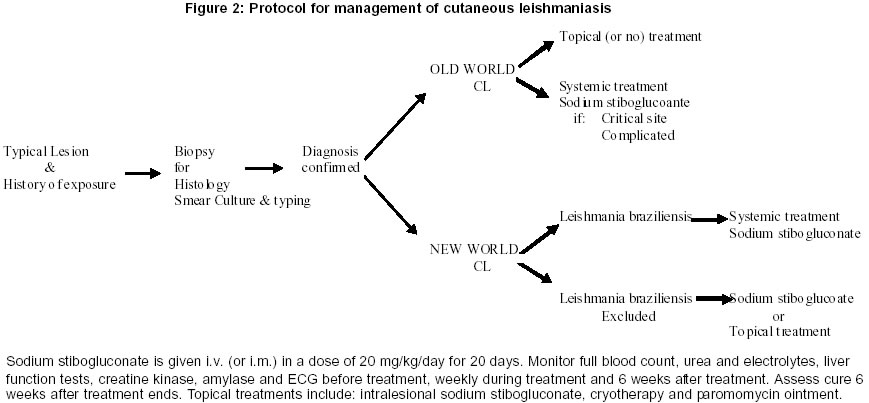
Code Number: jp03010 Abstract: Leishmaniasis is a major world health problem, which is increasing in incidence. In Northern Europe it is seen in travellers returning from endemic areas. The protozoa is transmitted by sandflies and may produce a variety of clinical syndromes varying from a simple ulcer to fatal systemic disease. This review considers the management of simple cutaneous leishmaniasis. Patients usually have a single ulcer that may heal spontaneously, requiring only topical, or no treatment at all. Lesions caused by Leishmania braziliensis may evolve into the mucocutaneous form, `espundia', and should be treated with systemic antimony. Sodium stibogluconate 20mg/kg/day i.v. for 20 days is the appropriate first line treatment in these cases. Although it may cause transient bone marrow suppression, liver damage, a chemical pancreatitis, and disturbances in the electrocardiogram, it appears safe. The success of treatment should be assessed 6 weeks after it has been completed and patients should be followed up for 6 months. (J Postgrad Med 2003;49:50-54) Key Words: Cutaneous leishmaniasis, treatment, stiboglucoanate. Cutaneous Leishamaniasis, first descriptions of which can be traced back to the 9th century (Balkh sore), remains a major world health problem in the 21st century. The Leishmaniases are caused by the protozoa leishmania, which is transmitted by the bite of an infected female sandfly. The result of infection can vary from a chronic skin ulcer, to erosive mucosal disease with progressive destruction of the nasopharynx and severe facial disfigurement, to a life threatening systemic infection with hepato-splenomegly. The resulting syndrome depends upon a complex interaction between a specific species of leishmania and the genetic and immunological status of the host (Figure 1). Epidemiology There are about 1.5 million new cases of cutaneous leishmaniasis (CL) each year of which over 90% occur in Afghanistan, Algeria, Iran, Iraq, Saudi Arabia, Syria, Brazil and Peru.1 However, CL often occurs in specific pockets not only of place but also in time for example Delhi boil affected 40,000 people in the early 1940s but is rarely seen in Delhi today. The geographical distribution of CL is mainly determined by the sandfly vectors (Phlebotomus sp and Lutzomyia sp). They live in dark, damp places, and are relatively weak flyers, with a range of only 50 metres from their breeding site. Unlike mosquitos, they fly silently and their small size (2-3mm long) allows them to penetrate mosquito nets. They are most active in the evening and at night. Sandfly numbers are related to natural factors such as rainfall,1,2 and may increase with global warming. Decreased insecticide spraying for malaria, poor waste disposal and heaps of construction waste encourage breeding has led to an increase in the prevalence of peri-domestic cases.3,4 Most infections exist as zoonoses amongst wild animals, such as rodents and dogs, and are most prevalent in rural or forest areas. Whilst man is usually an incidental host, such infections are by no means uncommon in endemic areas up to 9% of the healthy population may have positive leishmanin skin test - indicative of an earlier, often asymptomatic, infection.5 In India simple CL is usually due to L. tropica and man is the most common reservoir. In India Post Kala Azar Dermal Leishmaniasis (PKDL) is the most common cutaneous manifestation of leishmaniasis. Although not a strictly a form of CL it is important particularly in North Eastern India (particularly in Bihar State) where Visceral Leishmaniasis is epidemic.6 This type occurs in patients who were treated for visceral leishmaniasis, caused by L. donovani, some months or years earlier. The aetiology is unknown but possibilities include inadequate treatment or re-infection of patients previously cured of visceral leishmaniasis. Lesions are variable but often consist of hypo-pigmented macules, papules or nodules; they do not ulcerate, and may persist for months or years. These patients may play an important role as reservoirs of infection.7 In Southern Europe, where leishmaniasis is endemic, the incidence of visceral disease is increasing, often in association with HIV-1 infection. Many such patients develop unusual cutaneous manifestations.8,9 In North America and Northern Europe CL is a disease seen in returning travellers, such as those conducting rural field studies, tourists and the military. Unfortunately many of those infected are ignorant of the risks, take no personal protective measures and experience delays in diagnosis followed by inappropriate treatment upon their return.10 Pathology The life-cycle consists starts with inoculated promastigotes which are phagocytosed by macrophages, once inside they loose their flagella and become amastigotes which multiply by binary fission. Infected macrophages then burst, releasing their amastigotes to infect other macrophages. The subsequent fate of the amastigotes depends upon parasite and host factors, which are poorly understood. Viscerotrophic species, such as L. donovani, migrate throughout the reticulo-endothelial system, giving rise to visceral leishmaniasis; whereas dermotrophic species, such as L. major, usually remain close to the inoculation site, causing cutaneous disease. Any spread of dermotrophic species tends to be late, and only to adjacent skin (producing satellite lesions), or to lymphatics and regional lymph nodes. These phenotypic distinctions are not absolute. L. braziliensis is able to migrate to the oropharyngeal mucosa where it may remain dormant for many years before reactivating to cause the destructive mucocutaneous form `espundia'. There are reports of L. tropica causing visceral disease.11 In post-kala-azar dermal leishmaniasis the viscerotrophic parasite becomes dermotrophic as a consequence of treatment,12 as it may in those with HIV infection.9 In all forms of leishmaniasis the presence of amastigotes within the cells of the mononuclear phagocytic system remains the hall mark of the disease, although at times they may be difficult to detect. Infected macrophages measure 20-30 mm across whereas amastigotes (known as Leishman-Donovan bodies) are round to oval structures measuring only 2-5 mm. They are surrounded by a plasma membrane and contain both a relatively large, deeply basophilic, nucleus and a smaller, deeply staining, rod-shaped kinetoplast of extra-nuclear DNA (from the base of the flagellum which is lost in the conversion from promastigote to amastigote). Although H & E will demonstrate amastigotes, a Giemsa stain is preferred by many - as it stains the flagellum bright red.13,14 In early cutaneous lesions, the dermal infiltrate is mainly made up of macrophages filled with amastigotes. There are relatively few lymphocytes and plasma cells. As the lesion develops more lymphocytes and plasma cells appear and the superficial dermis becomes oedematous. The overlying epidermis becomes hyperkeratotic and subsequently breaks down to form an ulcer covered with a coagulum of hyperkeratotic debris, dried exudate, dead cells and a mixture of live and dead organisms. Over the following months, there is a gradual decrease in the number of amastigotes and macrophages, leaving a granulomatous infiltrate consisting of lymphocytes, epithelioid cells and multinucleate giant cells. At this stage it may be difficult or impossible to detect organisms in H&E, or Giemsa, stained sections. Ultimately, either the patient's immune response is able to eliminate the infection and effect a spontaneous cure, or it fails and a chronic form of leishmaniasis develops. Clinical Features Infection, following a bite from an infected sandfly, may remain sub-clinical or develop, after an incubation period of 1 to 12 weeks, into a papule that enlarges and then ulcerates. A typical lesion is a painless ulcer with a raised, indurated, margin and a necrotic base that is often covered with an adherent crust of dried exudate. Most patients have 1 or 2 lesions, usually on exposed sites, varying in size from 0.5 to 3 cm in diameter.15 There is, however, considerable variation: some lesions do not ulcerate, others develop sporotrichoid nodular lymphangitis. Secondary bacterial infection is common which can lead to pain. Most lesions heal over months or years, leaving an atrophic scar. In general half those lesions caused by L. major or L. mexicana will have healed in 3 months, those caused by L. tropica take longer about 10 months - and those due to L.brazilinesis persist much longer.16,17 Natural resolution leads to partial resistance to re-infection.18 Diagnosis The diagnosis is often made on the basis of a clinically typical lesion in conjunction with an appropriate history of exposure. However, there are a number of mimics (Table 1), and the treatment may be toxic, so pathological confirmation should be sought - preferably by demonstrating the organism in tissue and /or culture. Unfortunately this is not always possible in practice. In a study of 475 cases due to L. major in Saudi Arabia the parasite was demonstrated by smear in 50-80% (depending on the investigator and the technique used), by skin biopsy in 70% and by culture in only 50%. When all 3 methods were combined the parasite was still not detected in 10-20% of cases.19 The problem is often greater in New World disease, particularly in lesions over 6 months old.20,21 The best approach is to use several methods. Take a full thickness biopsy from the infiltrated margin of the lesion and divide it into 3 parts: to prepare an impression smear, for histological examination and for culture. Try to select a lesion, which is not secondarily infected, clean it thoroughly with 0.9% saline, or 70% alcohol, to remove the crust and any pus. If infection is present, a second clean with 6% hydrogen peroxide is helpful prior to injecting 2% lignocaine with adrenaline. Although a punch may be used, I prefer an elliptical biopsy taken with a scalpel. Haemostasis is achieved by pressure as sutures generally pull through. Impression smears are made by gently pressing the skin biopsy against a glass microscope slide 4-5 times after which the slide is dried in air then fixed in 95% ethanol for 3 minutes. They can then be stained with Giemsa or H & E and examined for the presence of amastigotes. Specimens for culture should be transported in `sloppy Evans' media and subsequently cultured on Evans Modified Tobies media or NNN media.22 Cultured organisms may be typed by isoenzyme analysis.22 Alternative methods of obtaining tissue for diagnosis include needle aspirates and slit skin smears. A needle aspirate is obtained by using a 2ml leur lock syringe with a 20 gauge needle, containing 0.3ml 0.9% saline. The needle is inserted through intact skin and 0.1 ml is injected into the edge of the lesion. The needle is then moved back and forth rotating it and applying suction at the same time to cut small pieces of tissue from the edge of the needle track, which are then aspirated. The aspirate can be used to inoculate cultures and prepare smears. Slit-skin smears are made by squeezing the edge of the lesion between thumb and forefinger, making a shallow slit 1mm deep in the pinched skin with a scalpel and then scrapping the cut edge.22 Attempts have been made to utilise molecular technology to improve diagnostic speed, convenience and specificity -but they remain research tools. Monoclonal antibodies can demonstrate parasites in paraffin sections but are often species specific.23 PCR methods are useful for confirming the diagnosis and offer improved sensitivity over microscopy and culture,24 however, problems exist with the identification of individual species, particularly causing American CL. Serology is unhelpful for cutaneous disease because antibodies tend to be undetectable or present in low titre.6 The Leishmanin skin test, which is analogous to the tuberculin test, detects cell-mediated immunity; becomes positive once the lesions begin to crust and remains so indefinitely. It cannot distinguish between past and present infection.5 Treatment There is no single optimal treatment for all forms of CL. Indeed, the natural diversity of the parasites, together with the wide spectrum of clinical disease that they produce, means one is unlikely to evolve in the foreseeable future. In an ideal world each endemic area would establish its own optimum treatment regimen based on efficacy and toxicity, without neglecting the practical difficulties of administration and cost. In reality data tends to be extrapolated from one situation to another with variable results. The situation is complicated by the self-healing nature of CL. Adequately controlled therapeutic trials are therefore essential to assess the efficacy of any new treatment. Unfortunately, the literature abounds with reports of `effective' treatments, based on case reports and uncontrolled, small, series making it difficult to assess their efficacy. Fortunately, there are some guiding principles. Lesions due to different species vary in both their severity and response to treatment American CL tends to be more severe and longer lasting than Old World CL. As most Old World lesions heal rapidly without treatment an expectant approach may be appropriate particularly for those patients living in endemic areas because spontaneous healing is associated with the development of protective immunity. Lesions on cosmetically or functionally important sites, such as the face or hands, those with associated lymphangitis and those with multiple or persistent lesions are best given active treatment. Local treatment is appropriate for those with early non-inflamed lesions and systemic therapy for those with multiple or more complicated lesions. In American CL the crucial first step is to decide whether or not L.braziliensis could be the infecting organism because, until further information is available, all such cases must be considered capable of progressing to mucocutaneous disease and therefore require adequate systemic therapy. Hence, if the patient contracted CL in any area in which L.braziliensis occurs (i.e. Belize, Colombia, Costa Rica, Guiana, Honduras, Surinam, Panama, Venezuela, the western slopes of the Andes and the Argentinean highlands),25 the parasite must be identified before alternatives to optimal systemic therapy can be considered. The pentavalent antimony derivatives sodium stibogluconate (Pentostam,Glaxo Wellcome, UK) and meglumine antimoniate (Glucantime, Rhone-Poulenc Rorer, France), developed in the 1940s, remain the mainstay of systemic treatment. They are similar in both efficacy and toxicity any reported differences can be explained by their differing antimony concentrations (Pentostam 100mg/ml; Glucantime 85mg/ml). Their mode of action is not known, although they inhibit glycolysis and fatty acid oxidation in leishmania.7 Their efficacy is well established - provided they are given in adequate doses and for an adequate length of time.16,26 In American CL sodium stibogluconate, 20mg/kg/day for 20 days is an appropriate course curing over 90% of cases in a single course.6,15,27,28 Shorter courses may be adequate for Old World disease. It is best given once daily by slow i.v.(or i.m.) injection. Toxicity is common, and appears dose related, most patients develop malaise, anorexia, myalgia and arthralgia after 14 days treatment. This is associated with elevations in serum aminotransferases, a chemical pancreatitis, a mild leucopenia, thrombocytopenia, and flattening of the T-waves on the ECG. Treatment should be monitored but in most cases these abnormalities settle rapidly once treatment is stopped.16,27 Lesions become less indurated, flatten, then re-epithelialise as they respond to treatment. However, healing continues after treatment has stopped so the need for additional treatment should delayed for 4-6 weeks. This also allows patients to recover from the toxicity.28,29 A protocol is suggested in Figure 2. Rifampicin has been reported to be efficacious but there are no good controlled trials to support its use and furthermore its use in areas where tuberculosis and leprosy are endemic should be avoided.17 Alternative systemic agents include aminosidine (paromomycin), pentamidine and ketoconazole, but they have yet to find a place in routine clinical practice.7 The most promising oral drug today is miltefosine. In an open label study in Colombia, four weeks treatment with 133 and 150mg of miltefosine daily cured 100% and 89% respectively.29 Local and topical therapy is an important option for those patient not at risk of mucocutanous disease. Local injection of sodium stibogluconate, or meglumine antimoniate, is useful for early, non-inflamed lesions. Technique is important infiltrate 1-3ml around the lesion to produce complete blanching at the base. It may be repeated on alternate days or given weekly until they heal.16,30,31 Aminosidine (paromomycin) ointment (15% paromomycin, 12% methyl benzethonium chloride in white soft paraffin) applied twice daily for 10 days is effective for L.major.31 and may also be useful for L.mexicana.7 It causes considerable local irritation, but less irritant derivatives have been less effective. Cryotherapy is also useful for small lesions (<1cm diameter). Apply two 20s freeze-thaw cycles to the whole lesion, assess response at intervals of 3 weeks and repeat once or twice if necessary.31 Lesions can also be treated by local excision, curettage or by electrodessication but are probably associated with a higher risk of relapse.7 The most recent topical agent to be investigated is the topical immunomodulator, Imiquimod, which was developed to treat genital warts. It produced a 90% cure rate in patients who had failed to respond to antimonials alone when it was used in conjunction with antimonials in Peru.32 A treatment protocol is suggested in Figure 2. Follow-up Patients should be monitored until the lesions have fully healed and the infiltration has resolved. Most relapses occur within 3-6 months after successful treatment,15,31 so follow up at 6 months is appropriate. Thereafter patient should be warned that relapse is possible and observe their scar for thickening, crusting or ulceration. Those who relapse should be given a full course of systemic antimony in the first instance. References
Copyright 2003 - Journal of Postgraduate Medicine. Online full-text also available at http://www.jpgmonline.com/ The following images related to this document are available:Photo images[jp03010t1.jpg] [jp030100f1.jpg] [jp03010f2.jpg] [jp03010f1.jpg] [jp030104f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}