 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 49, No. 1, Jan-March, 2003, pp. 55-60 Symposium Recent Advances in the Diagnosis of Leishmaniasis Singh S, Sivakumar R Division of Clinical Microbiology, All India Institute of Medical Sciences,
New Delhi - 110029, India.
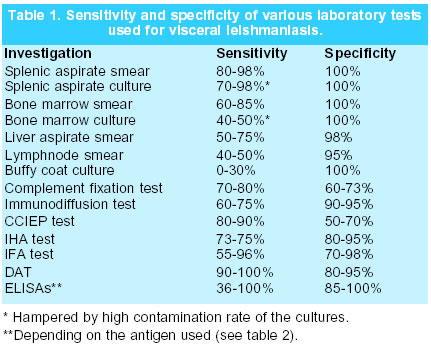
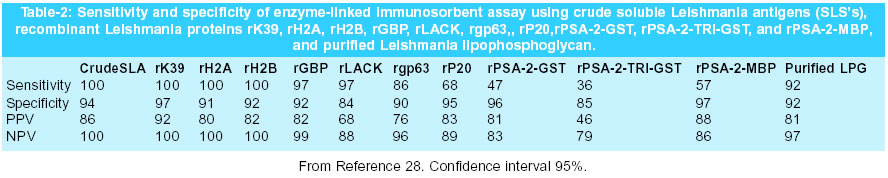
Code Number: jp03011 Abstract: Leishmaniasis is a parasitic disease caused by a haemoflagellate Leishmania. There are more than 21 species causing human infection. The infection is transmitted to humans through the bites of female sandflies belonging to 30 species. The disease manifests mainly in 3 forms: the visceral, the cutaneous and the mucocutaneous leishmaniasis. The diagnosis of visceral form is conventionally made by the demonstration of amastigotes of the parasite in the aspirated fluid from the bone marrow, the spleen, and rarely from the lymph nodes, or the liver. The parasite demonstration and isolation rates are rather poor from cutaneous and mucocutaneous lesions due to low parasite load and high rate of culture contamination. Recently several recombinant proteins have been developed to accomplish accurate diagnosis. Recombinant kinesin protein of 39 kDa called rK 39 is the most promising of these molecules. The antigen used in various test formats has been proved highly sensitive and specific for visceral leishmaniasis. It is useful in the diagnosts of HIV-Leishmania co-infection and as a prognostic marker. Molecular techniques targeting various genes of the parasite have also been reported, the PCR being the most common molecular technique successfully used for diagnosis and for differentiation of species. (J Postgrad Med 2003;49:55-60) Key Words: Leishmaniasis, Leishmania-HIV co-infection, diagnosis Leishmaniasis is a vector borne parasitic disease caused by a haemoflagellate, Leishmania spp. transmitted by the bite of infected phlebotomine sandfly. Depending on the causative species, it can manifest as Cutaneous Leishmaniasis (CL), Mucocutaneous Leishmaniasis (MCL), Diffused Cutaneous Leishmaniasis (DCL) or Visceral Leishmaniasis (VL). Leishmaniasis is prevalent in at least 88 countries. More than 90 percent of the cutaneous cases occur in Afghanistan, Saudi Arabia, Algeria, Brazil, Iran, Iraq, Syria and Sudan; while more than 90 percent of visceral cases occur in India and Sudan. Mucocutaneous form is mostly found in Latin America.1,2 Approximately 350 million people live in the area of active parasite transmission. Though several animal reservoirs have been identified in different countries for leishmaniasis, no animal reservoir of the parasite has yet been identified in India. It is presumed that skin lesions of a late sequel of the visceral form called post-kala-azar-dermal leishmanisis (PKDL) act as reservoirs.1,2 The clinical and epidemiological findings in various forms of leishmaniases are non pathognomonic and these can mimick several other conditions. Hence a laboratory diagnosis is required to confirm the clinical suspicion. The diagnostic tools used for each leishmanial syndrome viz. visceral, cutaneous, and mucocutaneous form vary but the gold standard in each case remains to be the demonstration and isolation of the parasite from appropriate tissues. Parasitological Diagnosis The differential diagnosis for VL includes, among others, malaria, tropical splenomegaly syndrome schistosomiasis, cirrhosis with portal hypertension, African trypanosomiasis, milliary tuberculosis, brucellosis, typhoid fever, bacterial endocarditis, histoplasmosis, malnutrition, lymphoma, and leukaemia. Similarly numerous primary and secondary skin diseases and conditions are frequently misdiagnosed as early lesions of cutaneous leishmaniasis. Some of the common conditions that should be differentiated from cutaneous leishmaniasis are tropical ulcers due to other causes, impetigo, infected insect bites, leprosy, lupus vulgaris, yaws, blastomycosis, and skin cancer.1,2 Mucocutaneous leishmaniasis is sequelae of new world cutaneous leishmaniasis and results from direct extension or hematogenous or lymphatic metastasis to the nasal or oral mucosa. Paracoccidioidomycosis, polymorphic reticulosis, Wegener's granulomatosis, lymphoma, histoplasmosis, yaws, tuberculosis, nasopharyngeal carcinoma, and other destructive lesions are frequently misdiagnosed as early lesions of mucocutaneous leishmaniasis.1-3 Hence other diagnostic methods are required to confirm the clinical suspicion.1,4 The diagnosis of leishmaniasis is reliably made by the demonstration of the parasite in smears and by isolation, either in culture or by animal inoculation of a biopsy sample or tissue aspirate from the spleen, or the bone marrow. The sensitivity is highest for splenic aspiration (as high as 98%) but so is the risk of complications such as haemorrhage. Occasionally the amastigotes have also been demonstrated in liver biopsy (50-85% sensitive), lymph node aspirates and buffy coat smears, particularly in HIV-Leishmania co-infection cases.1-4 The details are shown in Table 1. The parasitological diagnosis of CL is made by demonstration of amastigotes in skin lesions on skin biopsy and on culture of these specimens.1,2 Many other methods for demonstration of parasites such as histochemical and immunohistochemical examination of smears have been described.6-7 Culture based diagnosis of mucocutaneous leishmaniasis has very low sensitivity as the organisms are often scant.7 The individual sensitivities for the methods for patients and Montenegro-positive healthy controls were: histopathology: 14% and 16%; impression smear: 19% and 21%; dermal scraping: 22% and 26%; aspirate-culture: 58% and 64%; aspirate-hamster: 38% and 41%; biopsy-culture: 50% and 55%; and biopsy-hamster 52% and 57%, respectively. The sensitivity is slightly better for younger lesions than for lesions older than 6 months.8 Primary isolation of L. donovani is made on solid Novy- MacNeal- Nicolle (NNN) medium having 20-30% rabbit blood or liquid Schneider's insect medium supplemented with 10% v/v foetal calf serum (FCS). Other suitable growth media can also be used, particularly for maintaining the subcultures of the promastigotes using FCS or other supplements including human urine.5 Serological Diagnosis The biggest problem with conventional smear or culture techniques is low sensitivity particularly in detecting the occult and sub-clinical infections. These techniques are also cumbersome, and time consuming, and not suitable for field. The serological diagnosis is based on the presence of specific humoral response, as in cases of visceral leishmaniasis or cell mediated immune response, as in cases of cutaneous and mucocutaneous leishmaniasis.1 A wide range of serological methods varying in sensitivity and specificity are available for the diagnosis of VL. These serological methods can be grouped into non-specific and specific tests. The non-specific tests had been in use in the past but are very rarely used these days. A positive test does not confirm the diagnosis of Leishmaniasis.1 Indirect haemagglutination (IHA), counter-current immunoelectrophoresis (CCIEP), and Immunodiffusion (ID) are examples of non-specific tests. These tests are cumbersome and have lower sensitivity and specificity and hence not commonly used.8-10 Some more commonly used ones are described below. Leishmanin Skin Test (LST) Delayed hypersensitivity is an important feature of cutaneous forms of human leishmaniasis and can be measured by the leishmanin test, also known as the Montenegro reaction. Leishmanin is a killed suspension of whole (0.5-1 x 107/ml) or disrupted (250 µg protein/ml) promastigotes in pyrogen-free phenol saline. No cross-reactions occur with Chagas' disease, but some cross-reactions are found with cases of glandular tuberculosis and lepromatous leprosy. Leishmanin Skin Test is usually used as an indicator of the prevalence of cutaneous and mucocutaneous Leishmaniasis in human and animal populations and successful cure of visceral leishmaniasis.9,11,12 During active kala-azar disease there will be no or negligible cell mediated immune response. However, the leishmanin antigen is not commercially available and no field study has been carried out in India. Indirect Fluorescent Antibody Test (IFAT) The Indirect fluorescent antibody test is one of the most sensitive tests available. The test is based on detecting antibodies, which are demonstrated in the very early stages of infection and are undetectable six to nine months after cure. If the antibodies persist in low titers, it is good indication of a probable relapse. Titers above 1:20 are significant and above 1:128 are diagnostic.5 There is a possibility of a cross reaction with trypanosomal sera. However, this can be overcome by using leishmania amastigotes as the antigen instead of the promastigotes.10 Although this test is more sensitive (96%) and specific (98%) than soluble antigen ELISA, it is cumbersome and not suitable for field conditions.13 Direct Agglutination Test The direct agglutination test (DAT) is a highly specific and sensitive test. It is inexpensive and simple to perform making it ideal for both field and laboratory use. The method uses whole, stained promastigotes either as a suspension or in a freeze-dried form. The freeze-dried form is heat stable and facilitates the use of DAT in the field. However, the major disadvantage of DAT is the relative long incubation time of 18 h and the need for serial dilutions of serum.14,15 Also, DAT has no prognostic value. The test may remain positive for several years after cure. Recently, Schoone et al15 have developed a fast agglutination-screening test (FAST) for the rapid detection (<3 hours) of anti-leishmania antibodies in serum samples and on blood collected on filter paper. The FAST utilises only one serum dilution leading to qualitative results. It offers the advantages of DAT based on the freeze-dried antigen, of the antigen, reproducibility, specificity and sensitivity. Direct agglutination test has been evaluated for the diagnosis of cutaneous leishmaniasis using L. major promastigotes and was shown to be highly specific and sensitive (90.5%).16 Enzyme Linked Immunosorbent Assay The Enzyme Linked Immunosorbent Assay (ELISA) is a valuable tool in the serodiagnosis of leishmaniasis. The test is useful for laboratory analysis as well as for field applications. However, the sensitivity and specificity of ELISA is greatly influenced by the antigen used (Table 2). More recently, several recombinant antigens like rGBP from L. donovani, rORFF from L. infantum, rgp63, rK9, rK26 and rK39 from L.chagasi 17-22 have been developed and tested. Of these, the rK39 antigen is found to be highly sensitive and predictive of onset of disease manifestation in VL patients. In contrast, it does not show detectable antibodies in cutaneous or mucocutaneous leishmaniasis. The antibody titres to this antigen directly correlate with active disease and have potential in monitoring the chemotherapy and in predicting the clinical relapse. In addition rK39 ELISA has a high predictive value for detecting VL in immunocompromised persons, like those with AIDS. A kit (InBios®, USA) using this antigen and based on lateral flow is now commercially available in the form of antigen-impregnated nitrocellulose paper strips adapted for use under field conditions. The rK39 strip test has been found highly sensitive and a reliable indicator of kala-azar in India.23-26 Due to lack of facilities and expertise to perform skin biopsy, smears and cultures the proper diagnosis of cutaneous leishmaniasis remains under reported. The use of serological tools in the diagnosis of CL has also been assessed by a number of studies. ELISA using few recombinant antigens viz., gene B protein (GBP) from Leishmania major, recombinant major surface glycoprotein, gp63, from L. major, and 2 recombinant proteins, T26-U2 and T26-U4, from Leishmania (Viannia) peruviana have been tried but have been found less suitable for diagnosing CL.16,27 Laboratory diagnosis of MCL has also taken a back seat and most of the cases are diagnosed (and obviously may be over-diagnosed) clinically. Table 2 shows comparative sensitivity and specificity of various ELISA based antibody detection techniques.28 Immunoblotting Most of the work concerning the use of immunoblotting in the diagnosis of leishmaniasis has been done on visceral leishmaniasis (VL). In cutaneous leishmaniasis, anti-leishmania antibodies though detectable, are present in low tibres. Hence Immunoblotting is not widely adopted for diagnosing CL. The biggest advantage of immunoblotting, as a general rule, is that various antigens expressed and antibodies recognised during the course of infection can be documented. It also has an added advantage of permanent documentation. However, the technique is not user-friendly and limited only to research laboratories.1,10,29,30 Antigen Detection The antigen detection is an ideal method of diagnosing an infection. Antigen levels are expected to broadly correlate with the parasite load as well. This method of diagnosis should be a better alternative to the antibody detection methods, particularly in the immunocompromised patients, where antibody response is very poor. However, detection of antigen in the patient's serum is complicated by the presence of high level of antibodies, circulating immune complexes, serum amyloid, rheumatoid factor and autoantibodies; all of which may mask immunologically important antigenic determinants or competitively inhibit the binding of free antigen. Though a few reports are published, no satisfactory antigen detection system is currently available.31 Recently, a latex agglutination test (KATEX) for the detection of leishmanial antigens in the urine of patients with VL is developed.32 The results obtained with KATEX using samples collected from patients of different foci of VL indicate that, the test works well regardless of the geographical origin of samples. The test had 100% specificity and sensitivity between 68-100%. Whether the test has applications for the detection of asymptomatic cases of VL and monitoring therapy is yet to be confirmed. There are no antigen detection systems currently available for CL and MCL. Molecular Methods Microscopy and culture have the limitations of low sensitivity and are time consuming. The immunological methods fail to distinguish between past and present infections and are not very reliable in immunocompromised patients. While the molecular approach is capable of detecting nucleic acids unique to the parasite, it would address these limitations. A variety of nucleic acid detection methods targeting both DNA and RNA have been developed. Amongst these, the PCR has proved to be a highly sensitive and specific technique. The PCR assay can detect parasite DNA or RNA a few weeks ahead of appearance of any clinical signs or symptoms. Different DNA sequences in the genome of leishmania like ITS region, gp63 locus, telomeric sequences, sequence targets in rRNA genes such as 18s rRNA and SSU-rRNA and both conserved and variable regions in kinetoplast DNA (kDNA) minicircles are being used by various workers. 33-37 The PCR-SSCP technique has been developed for the detection of sequence variation in rRNA genes within the L. donovani species. In addition, it can be performed easily and rapidly from clinical samples without prior need of cultivation of the parasite. PCR assay has also been used for post therapeutic follow-up and for detection of relapses among HIV-infected patients using SSU rRNA gene target. The use of fluorogenic real-time PCR using SSU-rRNA gene added with complete automation has made quantification of parasite burden possible. Besides it is a rapid, sensitive and highly specific test.32-36 Recently, primers developed by us (unpublished data) could differentiate the Indian strains causing VL and PKDL forms. An Alu-PCR-like amplification was performed from the cultured L. donovani isolates from VL and PKDL patients. The banding pattern of the PCR amplicons could clearly group all the PKDL strains in one group while VL strains had intra-species heterogeneity as reported by us earlier.38 The chronic CL patients constitute the greatest diagnostic challenge due to the low density of Leishmania parasites. For acute CL, dermal scrapings from the bottom of the ulcer may yield viable specimens for PCR. Recently, the sampling method has been further improved using cotton swab for diagnosis of CL. Collection of the exudative material is easy, painless and convenient for both the patients as well as the collectors compared with other sampling methods. The collection of exudates by cotton swab may be a better alternative to biopsy samples for the diagnosis of CL by PCR, especially in field conditions.39-42 A PCR-ELISA technique developed recently is reported to be sufficiently sensitive and specific for use as a diagnostic test in cases of mucocutaneous leishmaniasis. Using this technique, the percentage of detection was 83.3% in blood samples from clinically diagnosed cases. No false positive results were obtained.43 However, the use of PCR as a routine diagnostic method still requires a well-prepared laboratory and well-trained personnel. This hampers the feasibility of using this technique directly in the field.
Other Surrogate Markers There are a few surrogate markers that can be used in predicting the prognosis of the kala-azar. Besides increase in haemoglobin and total and albumin fraction of the serum protein there is consequent decrease in serum globulin after sucessful treatment. This also increases the albumin/globulin ratio. Other laboratory parameters include increase in total WBC count, and decrease in ESR and serum levels of liver enzymes. The cytokines particularly, the TNF-alpha is another such prognostic marker. This cytokine is significantly raised in acute persistent cases of kala-azar but the levels come down sharply after parasitological cure.10 Leishmaniasis in HIV Infected Patients HIV modifies the clinical presentation of leishmaniasis in the co-infected patient. Several atypical etiologic agents have been described in leishmanial syndromes affecting HIV-infected subjects. HIV-associated leishmaniasis is characterized by parasite dissemination to the skin (as in DCL), spread of the "non-visceralizing" species throughout the reticulo-endothelial system and spread to the atypical locations, as well. A review of current literature found that 20-40% cases had absence of splenomegaly. Lack of anti-Leishmania antibodies is a characteristic feature seen in these patients. Leishmania amastigotes are commonly found in Kaposi's sarcoma and herpes zoster cutaneous lesions when HIV infected patients develope VL. Leishmaniasis has also been reported presenting with a dermatomyositis-like eruption in three patients with AIDS.44 Though India has less experience of HIV-Leishmania co-infection the number of such cases is bound to increase in Bihar. We have seen about 10 cases at this institute. All were referred from Bihar or Uttaranchal. Usually the promastigotes can easily be seen in these patients due to heavy load of parasites. We have found high utility of anti-rK39 in these patients. References
Copyright 2003 - Journal of Postgraduate Medicine. Online full-text also available at http://www.jpgmonline.com/ The following images related to this document are available:Photo images[jp03011t2.jpg] [jp03011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}