 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 49, No. 2, April-June, 2003, pp. 114-117 Brief Report Human Immunodeficiency Virus Type 1 Infection in Patients with Severe Falciparum Malaria in Urban India Khasnis AA, Karnad DR Department of Medicine, King Edward Memorial Hospital, Parel, Mumbai - 400012, India.
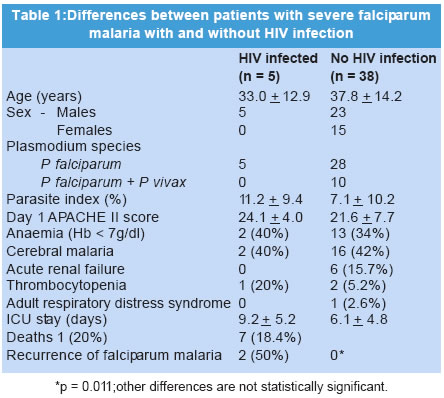
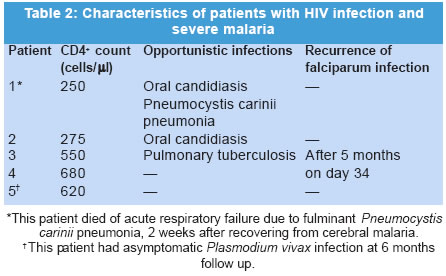
Code Number: jp03031 Abstract: BACKGROUND: CD4+ T cells restrict parasitaemia during the first attack of falciparum malaria; humoral immunity, develops weeks later and protects against reinfection. HIV infection may affect severity of falciparum malaria and development of protective immunity. AIMS: To study the prevalence of HIV infection in Indian patients with severe falciparum malaria and its effect on severity of illness and recurrences of and mortality related to malarial infection. PATIENTS: Consecutive patients with severe falciparum malaria and voluntary blood donors. SETTING AND DESIGN: Prospective cohort study in a university hospital in Mumbai. RESULTS: Five (11.6%) of 43 patients and 521 (1.8%) of 28749 blood donors had HIV infection (OR 7.1, 95% CI = 2.8 to 18.2, p=0.001). Clinical features, APACHE II score, number of organs affected, parasite index and mortality in patients with and without HIV infection were comparable. CD4+ counts were < 500 cells/μl in 2 patients and normal in 3. Opportunistic infections including pulmonary tuberculosis in one patient (CD4+ counts >500 cells/μl), and oral candidiasis in two (CD4+ counts 275 and 250 cells/μl) were noted. One patient developed fatal Pneumocystis carinii pneumonia two weeks after recovering from malaria. P. falciparum infection recurred in 2 of the 4 HIV infected survivors and in none of 31 survivors without HIV infection (RR 38.8, 95% CI 2.2 to 671, p=0.01). CONCLUSIONS: HIV infection is associated with increased risk of severe malaria even with normal CD4+ counts; severity of disease and mortality are not increased. However, prior HIV infection impairs protective immune response to Plasmodium falciparum in residents of hypoendemic areas. (J Postgrad Med 2003;49:114-117) Key Words: Plasmodium falciparum, acquired immunodeficiency syndrome, cell-mediated immunity, cerebral malaria, immunocompromised state, opportunistic infection Human immunodeficiency Virus (HIV) predominately affects the CD4+ T lymphocytes.1 These cells play an important role in immunity against Plasmodium falciparum infection.2-4 Two distinct types of CD4+ helper T cell responses have been identified based on cytokine secretion. One type, called TH1-type response, results in the production of interleukin 2 and interferon γ and activates the cellular arm of the immune system. Naive T cells typically exhibit such a response.2,5 A TH2-type response elicits production of other cytokines that activate a humoural response and is better seen in memory T cells.2,5 In individuals developing falciparum infection for the first time, the initial response is of the TH1-type, causing destruction of parasites via toxic mediators produced by activated macrophages.2,5 A TH2 type response is seen 18-60 days after the initial infection. The latter response may play little role in recovery from the acute infection, but induces production of protective antibodies that prevent parasite proliferation during subsequent reinfection by blockade of merozoite invasion of RBCs, antibody mediated cellular inhibition (ADCI) and by promoting opsonisation of infected erythrocytes.5 A switch to a predominant TH2 response at the cost of the TH1 response occurs at an early stage in the course of HIV infection,6 and could theoretically predispose an HIV-infected individual to severe malaria.2 Fatal malaria often develops in monkeys infected with the simian-human immunodeficiency virus.7 Although some studies in African patients with HIV infection have shown no increase in prevalence of asymptomatic parasitaemia,2,8,9 data on HIV infection and severe falciparum malaria is limited.1 We, therefore, prospectively studied prevalence of HIV infection and its impact on severity of infection and outcome in patients with severe falciparum malaria in Mumbai (Bombay). Patients and Methods All patients with severe falciparum malaria admitted to the ICU of the King Edward VII Memorial Hospital, a tertiary referral centre and university hospital during a 6-month period were studied after obtaining informed consent, using a protocol approved by the institution's ethics committee. The diagnosis of malaria was confirmed by the presence of ring forms of P falciparum in peripheral blood smears. Severe malaria was diagnosed using the WHO criteria.10 Patient characteristics, clinical course and outcome were noted. Blood was tested for HIV-1 antibody by microwell ELISA and HIV-1 infection was confirmed by western blotting. CD4+ counts were performed in all HIV seropositive patients soon after admission. Viral load was not estimated and none of the patients received any anti-retroviral treatment. Patients were treated for severe malaria with quinine (600 mg thrice daily for 7 days). Patients who had adverse effects with quinine received intra-muscular artemether. Intensive medical care was provided to all patients. No antimalarial chemoprophylaxis was advised after discharge from hospital. All patients were followed up by clinical and peripheral smear examination for 4 weeks for resistant malaria, and up to 6 months for development of reinfection. The prevalence of HIV seropositivity by ELISA in healthy voluntary blood donors from the blood bank of the hospital was considered to represent the prevalence of HIV infection in the city. Differences between groups were statistically compared using the student t test, chi-square test or the Fisher exact test (as applicable) and p < 0.05 was considered significant. Results HIV antibodies were detected in 521 (1.8%) of 28749 voluntary blood donors screened in the study period and in 5 (11.6%) of 43 patients with severe falciparum malaria (OR 7.1, 95% CI 2.8 to 18.2, p = 0.001). Age, parasite index and severity of illness as assessed by the Day 1 APACHE II score and number of organs affected were similar in patients with and without HIV infection (Table 1). None of the patients had co-infection with P vivax. In-hospital mortality and length of stay were comparable in both the groups (Table 1). CD4+ counts were normal in 3 patients and reduced in 2 (Table 2). Opportunistic infections were seen in 3 of the 5 patients with HIV infection (Table 2) and in none of the patients who were HIV seronegative (p = 0.0008). One patient developed severe Pneumocystis carinii pneumonia with acute respiratory failure 14 days after recovering from cerebral malaria and died 8 days later. During six months of follow up, recurrence of P falciparum malaria occurred in none of the 31 HIV seronegative subjects. However, 2 of the 4 HIV-infected survivors developed malaria (relative risk = 38.8, 95% CI 2.2 to 671, p = 0.011). One patient with HIV infection (Patient 4) developed high fever, delirium, impaired consciousness and reappearance of parasitaemia 34 days after the initial malarial infection. He was readmitted and treated for cerebral malaria with parenteral quinine. Patient 3 developed fever 5 months after discharge. His peripheral blood smear showed trophozoites of Plasmodium falciparum with a parasitic index of 3%. Another patient (Table 2, Patient 5) was found to have asymptomatic parasitaemia with Plasmodium vivax when he came for follow-up at the end of 6 months. There was no correlation between the peripheral blood CD4+ counts and recurrence of malaria (Table 2). Discussion Although HIV infection is estimated to affect approximately 0.8% of Indians,11 its prevalence in non-high risk adults is not known. We, therefore, studied the seroprevalence in voluntary blood donors and found that 1.8% of blood donors were seropositive. This is consistent with the 1.81% prevalence reported from another blood bank in Mumbai.12 When compared with voluntary blood donors, the prevalence of HIV infection was significantly higher (11.6%) in patients with severe malaria, suggesting that malaria may be more severe in patients with HIV infection. HIV infection could perturb immune responses against P falciparum as a result of T-helper cell and macrophage dysfunction. A study from Uganda has shown that adult patients with AIDS have titers of antibodies against several plasmodial antigens which are below protective levels while titers in HIV seropositive patients without AIDS are comparable to those without HIV infection.13 Yet, several studies, together involving over 11000 African adults, have failed to show an increased incidence of asymptomatic parasitaemia or non-severe malaria in HIV infection.2,3,8,9 There is only one study that has investigated the relationship between HIV infection and severe malaria. This study carried out in Zambia demonstrated that prevalence of HIV infection in 27 Zambian adult patients with severe malaria no higher than that in patients admitted to the same unit for other diseases.14 The conflicting results of this study and our observations can be explained by differences in the epidemiology of severe falciparum malaria in Africa and Asia.10,15 Falciparum malaria has been endemic in Africa for several centuries and this region is considered to be hyperendemic.10,15 In hyperendemic areas, children develop natural immunity to falciparum infection by the time they are 5 years old.10,15-18 This immunity, presumably antibody-mediated, may not prevent re-infection but protects against high parasitaemia and severe infection; cerebral malaria is therefore rare in adults.15-17 Once established, antibody response can be maintained for several years in the absence of T cell help.2 Antibody titres in early HIV infection may actually be higher than those in normal adults as a result of the predominant TH2 response.13 Thus, HIV infection acquired after the development of protective immunity against Plasmodium falciparum, typically seen in African adults, may not increase the risk of developing symptomatic or severe malaria. Whether HIV infection acquired before development of natural immunity against P falciparum increases the severity of infection by interfering with the TH1 type T helper cell response is not clear.2 This question can be answered only by studies like the present one done in less endemic regions. In Africa, an analogous situation exists in children who have acquired HIV infection before getting falciparum malaria. In a study from Zaire only 2 of 169 children with severe malaria had HIV infection as compared to 1 of 169 healthy sibling controls, suggesting that HIV infection is not a risk factor for severe malaria in African children.17 However, most children in this study acquired HIV infection following blood transfusions presumably for haemolytic anaemia. Several haemoglobinopathies, which are common in Africa, confer some protection against plasmodial infection and could therefore have compensated for the effect of HIV infection to a variable extent.10,15 Moreover, the duration of HIV infection in these children (median age 3.5 years) may have been too short to produce immune dysfunction. Thus, it appears that HIV infection may not increase severity of falciparum malaria infection in hyperendemic regions because anti-plasmodial immunity develops before immunodeficiency manifests. Once acquired, this humoral immunity may persist despite severe immunodeficiency. In contrast, disease transmission is still unstable in tropical Asia and most adults do not possess natural immunity.14,16 Our study suggests that preceding HIV infection in these non-immune adults may predispose them to severe malaria. Five of our 43 patients with severe malaria had HIV infection. Only 2 of these patients had low peripheral blood CD4+ counts (< 500 cells/μl) and none had CD4+ counts less than the critical level of 200 cells/μl, below which opportunistic infections are common.19 Thus, unlike other opportunistic infections, malaria seems to occur in patients with normal or only mildly depressed CD4+ cell counts. However, while the prevalence of HIV infection in patients with severe malaria was higher than expected, it did not increase disease severity or mortality. The six months follow up results suggest that HIV infection may also interfere with development of natural immunity following falciparum infection. Although we did not measure protective antibody titers, the rate of recurrence of falciparum malaria was much higher in patients with HIV infection than in those without. In conclusion, the present study suggests that HIV infection may predispose to severe falciparum malaria in adult Asian patients. The response to treatment was not affected in these patients. The higher recurrence rate indicates an impairment of their ability to mount a sustained immune response against P falciparum, even when the CD4+ T lymphocyte counts in peripheral blood exceed 200 cells/μl. Larger longitudinal studies in a cohort of adults with HIV infection living in hypoendemic areas are needed to confirm our observations. Acknowledgements The authors thank Drs C V Patankar and D Mohanty for technical assistance, Dr Smita Bijoor for access to blood bank records and Drs Ramesh S Kamat and Philip Abraham for their valuable comments. References
Copyright 2003 - Journal of Postgraduate Medicine. Online full-text also available at http://www.jpgmonline.com/ The following images related to this document are available:Photo images[jp03031t1.jpg] [jp03031t2.jpg] |
| |||||||||

{kind=link}
{kind=link}