 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Postgraduate Medicine, Vol. 50, No. 1, January-March, 2004, pp. 35-39 Symposium The detection and treatment of Plasmodium falciparum malaria: Time for change Nosten F, Ashley E Centre for Vaccinology and Tropical Medicine, Nuffield
Department of Clinical Medicine, John Radcliffe Hospital, Headington,
Oxford
Code Number: jp04010 Abstract In most countries where malaria is endemic, P. falciparum malaria is on the rise. This is primarily due to the spread of drug-resistant strains. Drug resistance is mediated by spontaneous changes in the parasite genome that allow resistant parasites to escape the action of the drugs. The spread of drug resistance increases the transmission of malaria parasites. The consequences for the populations at risk are profound both in terms of consequences for health and economy. In order to halt the progression of drug resistance, we need to change the way antimalarials are used. As in tuberculosis and HIV/AIDS, we must use a combination of drugs for the treatment of malaria. Taking into account the pharmacokinetic and pharmacodynamic properties of the various anti-malarial agents, artemisinin-based combination therapy (ACT) seems to be the best option. This strategy should be used in conjunction with early diagnosis and appropriate vector control measures to achieve reduction in the emergence and spread of drug resistance.In all the major endemic regions of the world, including the Indian subcontinent, malaria is on the rise.[1] Consequently, the morbidity and mortality associated with this disease are worsening. In many countries these preventable negative impacts on the health are not documented and therefore ignored. In addition, malaria exerts a huge economic burden, by direct and indirect costs on the communities and the countries′ overall economy.[2] However, this economic burden too is often overlooked because it mainly affects the poorest segments of the society. The main reason for the worsening situation is the emergence and spread of multi-drug-resistant strains of P. falciparum. Over the last 30 years, all antimalarials (with the exception of the artemisinin derivatives) have fallen to resistance, one after the other, usually within a few years of the initial deployment. The "domino-like" strategy of using antimalarials in succession, and too often without prior confirmation of the diagnosis, has resulted in the present situation: we have lost almost all effective drugs to resistance and malaria is coming back with a vengeance. Unfortunately, manufacturing and marketing of antimalarial drugs may not be a profitable venture. Therefore, there are no new drugs ready for deployment. Similarly, a malaria vaccine, considered to be always around the corner, is unlikely to be available for several decades. Vector control measures are effective in areas of intense transmission but will not stop development of drug resistance. A new strategy is proposed, based on early detection and treatment with an artemisinin-based combination therapy (ACT). This new approach pioneered in South East Asia (SEA), has now been adopted by the W.H.O. and should be utilized in all endemic regions.[3] This paper summarises the basic principles of this new approach to malaria control and presents the existing evidence. Mechanisms of resistance It is believed that P. falciparum parasites become resistant to antimalarial drugs through spontaneous genetic mutations. These mutations are not induced by the drugs themselves, and for most drugs, the precise site of each mutation is not known. This is because the mode of action of most antimalarials is largely unknown or poorly understood. However, for certain antimalarials such as SP (sulfadoxine-pyrimethamine), the mutations that confer resistance to the parasite have been characterised. A series of mutations in the DHFR encoding gene will enable the parasite to survive the action of pyrimethamine. Successive mutations in the DHPS gene (on chromosome 8) will in turn confer resistance to the sulfadoxine component.[4] For drugs such as chloroquine (CQ), mefloquine and other quinolines (halofantrine, quinine), the mechanism of resistance is probably multigenic. The gene encoding for the protein pfCRT (chromosome 7) has been associated with resistance to chloroquine,[5] while mutations and number of copies of the gene encoding for pfmdr1 seem to be implicated in the resistance to mefloquine.[6] Because these mutations are spontaneous (and not induced), they are more likely to occur when there are large numbers of individual parasites (large parasite biomass) as during the acute phase of the disease. This is when the selection of resistant mutants occurs: the de novo selection.[7] On the contrary, during convalescence or in case of a new infection contracted during the elimination phase of a drug with a long half-life, parasites that already carry the mutation(s) conferring resistance will be "filtered" and will survive the low concentrations of the drug. This is, in fact, a mechanism of enhancement of resistance rather than selection. Finally, these mutations allowing the parasite to resist the action of the drug will be transmitted to other hosts by the gametocytes. The level of transmission, vector capacity, in-vector recombination of genes, and multiplicity of clones per infection, are all important factors that will influence the speed at which resistance will emerge and spread.Consequences of resistance Most of the time the consequences of resistance are not studied and are ignored. However, when they are studied, it is clearly seen that when resistance of P. falciparum increases and spreads, the following happens:
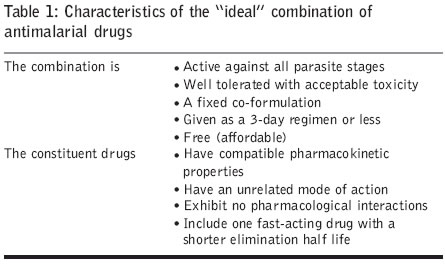
Combination therapy The concept of drug combinations is not new. Anti-infective drugs are combined to treat tuberculosis, leprosy and HIV, since it is believed that genetic mutations conferring drug resistance are less likely to occur simultaneously at different sites of the pathogen′s genome. For malaria, earlier combinations of antimalarials were developed without the precise knowledge of the pharmacokinetic and pharmacodynamic properties of the individual drug. In addition, antimalarials have clearly different speeds of action as far as parasite killing is concerned. This is illustrated in [Figure - 2], which shows the parasite reduction ratio (PRR) of various drugs. The PRR is the ratio of the parasite biomass at 48-hour intervals. For example, the artemisinin derivatives (QHS) can reduce the number of parasites in the body by a factor of 10[4] every cycle (48h), while antibiotics are much slower and can only reduce the number of parasites by a factor of 10 every cycle.In the treatment of uncomplicated malaria, the objective is to obtain a rapid reduction of the parasite biomass (to avoid clinical deterioration), complete elimination of all parasites in the patient (to avoid recrudescence) and finally, to reduce the possibility of transmission (to avoid the spread of resistance by the gametocytes). The necessary characteristics of the "ideal" antimalarial combination are summarized in [Table - 1]. It is clear that only the artemisinin-based combinations can fulfil these criteria. Unfortunately, the list of potential combinations is limited and none of them is "ideal" [Table - 2]. The most studied of the artemisinin-based combination therapies (ACT) is mefloquine-artesunate. More than 10,000 patients recruited in prospective trials have received this combination. It is safe and well tolerated but mefloquine is often associated with vomiting and dizziness.[13] The systematic use of this ACT with early diagnosis on the Thai-Myanmar border has resulted in a dramatic drop in the incidence of P. falciparum infections, and has halted the progression of resistance to mefloquine.[14] A fixed combination of artemether and lumefantrine (Coartem ®) has the necessary qualities for an effective ACT. However, the dosage schedule (twice a day for 3 days) might impair adherence to the treatment. In addition, it is required to be given with some fat, in order to be absorbed.[15] The 4 doses regimen sometimes suggested must be abandoned because this results in plasma concentrations of lumefantrine that are insufficient even in infections caused by sensitive isolates. Coartem ® is safe and well tolerated and effective against most resistant isolates.[16] Unfortunately, the price of the treatment (2.4 USD even when subsidised) is still too high. The combination of artesunate with SP or with amodiaquine (AQ) is potentially useful in areas where these drugs remain effective.[17],[18] Unfortunately, these are now limited to some countries in West Africa, while in Asia (including India, Pakistan and surrounding regions) most isolates have some degree of resistance to CQ and this resistance probably extends to AQ and to SP, as well. A new fixed combination- di-hydroartemisinin plus piperaquine-is now being studied in large trials and has shown promising results. It is as effective as mefloquine-artesunate, has a much better toxicity profile and the cost of an adult treatment course could be as low as 1 USD. [Table - 3] summarizes the dosages recommended for the various ACT regimens. Future ACT will include artesunate with pyronaridine or Lapdap ® (Lapdap-plus). Expectations and limitations of ACT All the available evidence suggests that ACT always improves clinical and parasitological recovery. This is due to the fast-acting artemisinin derivatives and is beneficial for the patients. On the Thai-Myanmar border, none of the 10,000 patients treated in trials with ACT experienced a deterioration of the malaria infection because of poor initial response to treatment. It is thus reasonable to expect that ACT will prevent the mortality caused by the rise of an uncontrolled parasite biomass. ACTs are also effective in reducing gametocyte carriage. This has been shown in all studies whether in Asia or in Africa. This means that ACT will reduce malaria transmission, especially in areas of low transmission (as shown in SEA) and will reduce the transmission of resistant strains in all areas. However, this has not been documented yet in areas of high transmission such as in sub-Saharan Africa. One should not expect ACT to dramatically reduce malaria transmission in sub-Saharan Africa because of the large reservoir of asymptomatic carriers. However, those patients with symptomatic infections who receive ACT would be less likely to transmit their potentially resistant infection to others and this is very significant. Unsuitable combinations The diagnosis of malaria In many endemic countries, the diagnosis of malaria is made on the basis of clinical symptoms. Algorithms have been developed to help in differentiating malaria from other diseases. However, the diagnosis of malaria is notoriously difficult because the clinical symptoms overlap with those of other diseases such as respiratory infections, dengue, leptospirosis and scrub typhus amongst others. As a result, antimalarials are being prescribed to patients who do not have malaria while others with malaria parasites, are left untreated. This clearly contributes to the overall cost of malaria and to the spread of resistance. Other factors such as under-dosing, poor adherence (encouraged by the perception that the prescribed medications are ineffective) and substandard drugs also contribute to the problem. Large-scale studies in Thailand, Cambodia and South Africa have shown that the biological confirmation of malaria by microscopy or by rapid tests is essential for a successful strategy of control.Peripheral smear microscopy remains the "gold standard" for the diagnosis of malaria and it should be used whenever possible. The advantages include high sensitivity and specificity for diagnosing malaria, its ability to identify the infecting malarial parasite species, and the potential use of the same technique for the diagnosis of other diseases, for example tuberculosis. On the down side, it is difficult to maintain quality control for good microscopy, it requires trained technicians and it is costly. The development of rapid diagnostic tests (RDT) has substantially improved the possibilities for the diagnosis of malaria. These tests are easy to use, reliable and inexpensive.[20],[21] The most useful amongst this group of tests are based on the detection of the parasite HRP2 protein or plasmodium lactate dehydrogenase, released by the infected red cells. To date, they remain too costly for the poorest patients and persistence of HRP-2 anti genemia limits their use. Thus, should not replace microscopy but rather be used when the latter is not possible. An important component of the new strategy is that the diagnosis (and treatment) of malaria (in particular when caused by P. falciparum) must be prompt. In practice, this means within 48 hours of the onset of fever. This short delay has been shown in field studies to allow the maximum reduction in gametocyte carriage by preventing the switch to gametocytogenesis. Hence, there will be a reduction in transmission and in the spread of resistant strains.[11],[14],[22] In order to permit such a short delay, the facilities for diagnosis and treatment must be available at the village and community levels. As Hackett declared long ago: "It is clear that the governments cannot rely on formula invented in Geneva or elsewhere, but they must create the mechanism simple and necessary to define and resolve their own problems, village after village".[23] Experimental deployment of such an approach was successful in reducing the incidence of malaria in the western border of Thailand and in South Africa. Discussion Malaria is back and its devastating health and economic consequences are mounting. This is particularly true in countries where most malaria cases are either untreated or treated with ineffective drugs. In SEA, the Indian subcontinent and the East Pacific region, CQ, AQ and SP are ineffective against P. falciparum. Some studies have found that these drugs may retain some efficacy[24] but often these trials are conducted in patients that may self cure (because of a transient immunity or premunition) and have too short a period of follow-up to detect late recrudescence. Mefloquine, quinine and the artemisinin derivatives remain effective so far, but we must be very cautious when using them so that they do not follow the same path to resistance. In order to protect the few remaining effective compounds, they must be used in combination. The most successful combinations of antimalarials are those containing an artemisinin derivative, especially artesunate. In SEA, countries such as Thailand, Cambodia, Laos and Myanmar have changed their malaria treatment policies and adopted mefloquine-artesunate as first line treatment. This is a step in the right direction but much remains to be done to make this treatment available to those who need it the most. Other countries (including those in Africa) have chosen to delay the change, mainly on economic grounds. This is probably an indication of short-sighted planning, because the real cost of malaria in many countries is already higher than the cost of changing (and delivering) therapy and this will only worsen as resistance spreads. Although still very insufficient, more money is now available for malaria programmes than ever before through the Global Fund for tuberculosis, AIDS and malaria, the World Bank, private foundations and governments and non-governmental organizations (NGOs). They are all contributing to this effort. The countries where malaria is worsening need to be supported to deploy comprehensive malaria programmes including early diagnosis and prompt treatment with an ACT. This is in line with the top priority for all malaria programmes since the Ministerial Conference in Amsterdam (1992). This strategy has been endorsed by the WHO/RBM recommendations but is not implemented. Instead much efforts and funds have been placed in impregnated bed nets. Although these barriers would have an impact in areas of intense transmission,[25] they would have only a limited impact in the areas of low and unstable transmission that prevail in Asia, which has the well described "mass killing" effect at the community level. It is sometimes suggested that the efficacy and tolerability of new antimalarial drugs should be assessed in each and every area before deployment. This is unrealistic and unnecessary for ACT. These regimens (mefloquine -artesunate, Coartem ®, Artekin ®) have been shown to be effective against the most resistant parasites in the world, so they should be effective everywhere. The safety of artesunate alone or in combination has been assessed in more patients than with any other antimalarial agent. Is anyone suggesting that the efficacy of anti-tuberculosis treatment or HAART be tested in each and every country? Why is malaria being treated differently? The time for change has come. It is essential to stop treating malaria cases with ineffective drugs and break the vicious circle of resistance. Otherwise we will lose the last drugs that we have and will be confronted in Asia, as in Africa, with a malaria disaster.[26] References
Copyright 2004 - Journal of Postgraduate Medicine The following images related to this document are available:Photo images[jp04010f2.gif] [jp04010t2.jpg] [jp04010f1.jpg] [jp04010t1.jpg] [jp04010t3.jpg] |
| |||||||||

![[Figure - 1]](/showimage?jp/photo/jp04010f1.jpg){kind=link}
![[Figure - 2]](/showimage?jp/photo/jp04010f2.gif){kind=link}
{kind=link}
{kind=link}
![[Table - 3]](/showimage?jp/photo/jp04010t3.jpg){kind=link}